Masayasu Aikawa, MD, Mitsuo Miyazawa, MD, Katsuya Okada, MD, Yasuko Toshimitsu, MD, Kojun Okamoto, MD, Shigeki Yamaguchi, MD, Isamu Koyama, MD. Saitama Medical University International Medical Center
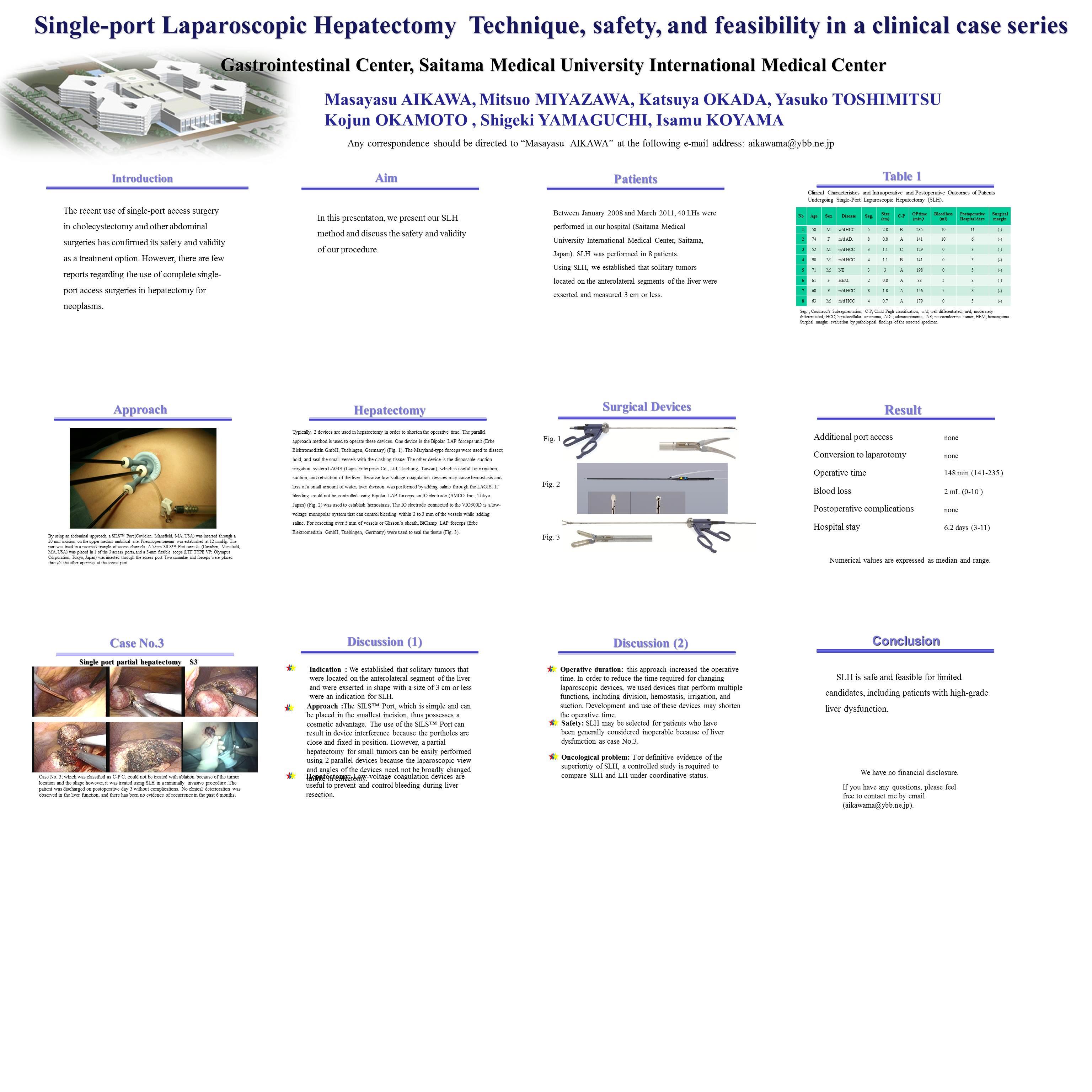
Background: The recent use of single-port access surgery in cholecystectomy and other abdominal surgeries has confirmed its safety and validity as a treatment option. However, there are few reports regarding the use of complete single-port access surgeries in hepatectomy for neoplasms.
Method: Between January 2008 and March 2011, 40 LHs were performed in our hospital (Saitama Medical University International Medical Center, Saitama, Japan). We performed single-port laparoscopic hepatectomy (SLH) in 8 patients, among whom 5 patients had hepatocellular carcinoma, 1 had metastatic liver tumor, 1 had endocrine liver tumor, and 1 had hemangioma. Further, 5 patients were classified in the Child-Pugh category A, 2 were in category B, and 1 was in category C. The tumors were located in the S2 in 1 patient, S3 in 2 patients, S4 in 2 patients, S5 in 1 patient, and S8 in 2 patients. The patients were eligible for SLH if they had solitary tumors measuring 3 cm or less on the caudal surface of the liver. In an abdominal approach, a SILS™ Port (Covidien, Mansfield, MA, USA) was inserted through a 20-mm incision on the upper median umbilical site.In hepatectomy, 2 devices are typically used in order to shorten the operative time. The parallel approach method is used to operate these devices. One device is the Bipolar LAP forceps unit (Erbe Elektromedizin GmbH, Tuebingen, Germany) , which is connected to the electrosurgical unit VIO300D (Erbe Elektromedizin GmbH, Tuebingen, Germany) for low-voltage coagulation. The other device is the disposable suction irrigation system LAGIS (Lagis Enterprise Co., Ltd, Taichung, Taiwan), which is useful for irrigation, suction, and retraction of the liver .
Results: No patient developed intraoperative complications that required additional port access and conversion to laparotomy. Operative time was 148 min (141-235 min). The postoperative course of the patients was uneventful, and they were discharged at an average of 6.2 days (3-11 days) after the operation. Approximately 2 weeks after discharge, the patients did not experience wound pain or liver dysfunction.
Conclusion: SLH is a safe and feasible procedure for a specific group of candidates, including patients with high-grade liver dysfunction.
Session Number: Poster – Poster Presentations
Program Number: P388
View Poster