Anjali Kumar, MD MPH, Kirthi Kolli, MBBS, Katherine Khalifeh, MD, James F Fitzgerald, MD. Washington Hospital Center
BACKGROUND: When designing investigations to address issues of obesity in rectal cancer patients, it is important to note that obesity is traditionally measured using the metric of body mass index (BMI – weight in kg/height in meters^2). BMI, however, may not be the most optimal assessment of obesity as it relates to rectal cancer. Men and women have inherent differences in the distribution of visceral (intraabdominal) versus surface area (extra abdominal) adiposity that contribute greatly to the technical challenges of proctectomy. We sought to investigate the differences in outcomes after resection for rectal cancer by type of operation undertaken, sex, and BMI
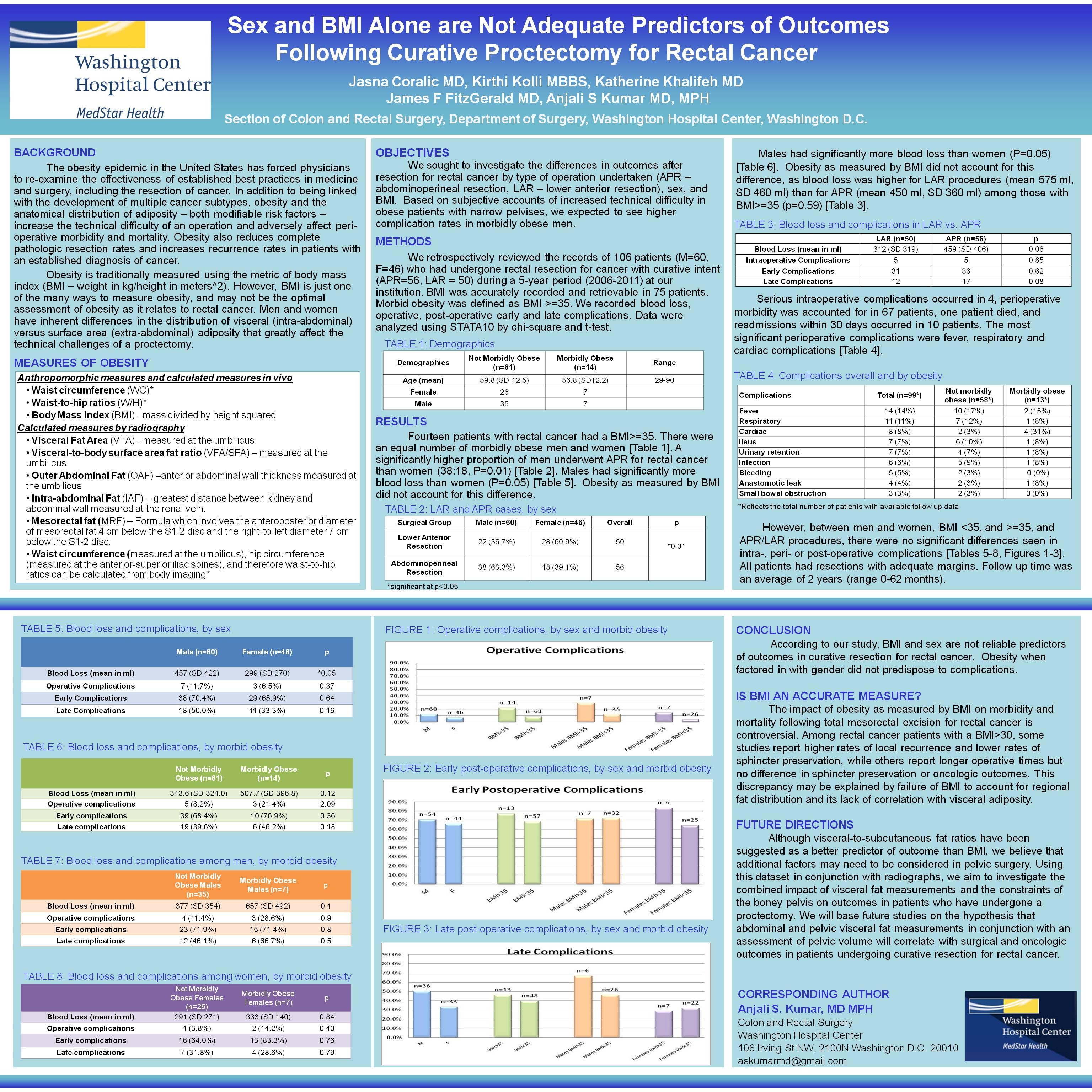
METHODS: We retrospectively reviewed the records of 92 patients (M=57, F=35) who had undergone rectal resection for cancer with curative intent (APR=52, LAR = 40) during a 5-year period (2006-2010) at our institution. Morbid obesity was defined as BMI >=35 and was accurately recorded in 69 patients. We recorded blood loss, operative, peri-operative and post-operative complications. We expected that obesity when factored in with gender would predispose to complications. Data were analysed using STATA10 by chi square and t-test.
RESULTS: 13 patients with rectal cancer had a BMI>=35. There was a higher proportion of morbidly obese men than women (5:8). A significantly higher proportion of men underwent APR for rectal cancer than women (37:15, P=0.04). Males had significantly more blood loss than women (P=0.05), and this could be explained by a significantly higher operative blood loss in APR procedures than in LAR (p=0.03). Obesity as measured by BMI did not account for this difference, as blood loss was higher for LAR procedures than for APR among those with BMI>=35. Serious intraoperative complications occured in 4, perioperative morbidity was accounted for in 59 patients, one patient died, and readmissions within 30 days occured in 10 patients. However, between men and women, BMI <35, and >=35, and APR/LAR procedures, there were no significant differences seen in intra-, peri- or post-operative complications, nor were there for recurrences, regardless of stage of cancer or implementation of neoadjuvant therapy. All patients had resections with adequate margins. Follow up time was an average of 2 years (range 0-62 months).
CONCLUSION: BMI and sex when analyzed independently are not reliable predictors of outcomes in curative resection for rectal cancer. Although visceral-to-subcutaneous fat ratios have been suggested as better predictors, bony pelvic constraints may also contribute, which we aim to investigate using this dataset in future collaborations with radiologists at our institution.
Session Number: Poster – Poster Presentations
Program Number: P063
View Poster