Tiffany C Cox, MD, Jonathan P Pearl, MD FACS, E. Matthew Ritter, MD FACS. National Capital Consortium Bethesda, Maryland
INTRODUCTION: Training to perform diagnostic colonoscopy is difficult to acquire. Currently there is no consensus on what constitutes competency in performing diagnostic colonoscopy. Virtual reality simulators have shown promise for assessing endoscopic skills, but at a significant cost. We present the initial development of a simulation based assessment tool to objectively evaluate the skill set required for diagnostic colonoscopy in a physical model.
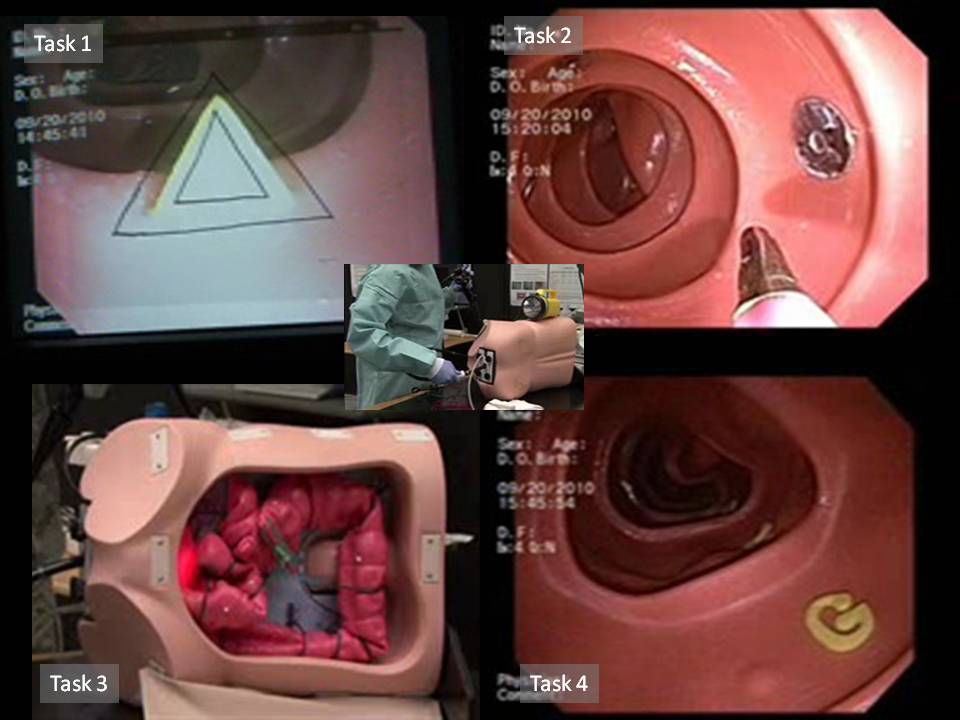
METHODS: Task analysis for diagnostic colonoscopy was performed by the authors to identify core skills. The identified skills were developed into 4 tasks using the Kyoto Kagaku colonoscopy model (Kyoto Kagaku Co Ltd, Japan). These include: 1) manipulation of the endoscope using torque and tip deflection including the ability to retroflex the scope, 2) performing basic biopsy techniques, 3) recognition and reduction of colonic loop formation, and 4) performance of a complete mucosal inspection. Task 1, scope manipulation, requires use of torque and tip deflection to align a shape in the colon with a matching shape on the monitor screen. Task 2, tool targeting, requires coordination with biopsy forceps to contact a metal target, completing a circuit and turning on a light. Task 3, loop reduction, requires reduction of a standardized alpha loop with navigation to the cecum. Task 4, mucosal inspection, requires identification of subtle polyps placed randomly throughout a length of simulated colon and rectum requiring careful mucosal inspection, including retroflexion. The SCOPE assessment tool was evaluated with a survey for face and content validity by a panel of experts in the field of general surgery, colorectal surgery, and gastroenterology.
RESULTS: A functional prototype of the assessment tool was created using two separate lengths of simulated colon, each representing 2 tasks. One task is performed during the insertion phase and the other during withdraw phase for each colonic segment. The simulator was evaluated for face and content validity by our experienced group using a 5-point Likert scale. The main focus of the survey was the realism of the simulator and the accurate representation of the skills required to perform diagnostic colonoscopy. Ninety two percent felt that overall the simulator was realistic. With each task, 92-100% of the evaluators felt these core skills accurately represented skills required for diagnostic colonoscopy. All evaluators agreed the simulator was a useful tool in evaluating colonoscopy skills and would recommend this simulator to be a part of skills assessment program.
CONCLUSION: Our S.C.O.P.E. assessment tool is realistic and reflects the core skills necessary to perform diagnostic colonoscopy. With these promising results, the next step is to refine performance metrics and assess construct validity.
Session: Poster
Program Number: P184
View Poster
{kind=link}