NIAZY M SELIM, MD PhD MBChB FACS. UNIVERISTY OF KANSAS
Introduction: The surgical approach to PEH is a challenging one. Over the past decade, laparoscopic surgery became the standard approach for the repair of paraesophageal hiatal hernias (PEH). The difficulties originate from the depth of the hernia in the mediastinum as well as the narrow orifice (hiatus) to dissect beyond.
Herein, The author presents a novel study and one of the largest series for the robotic repair of 30 giant PEH involving the stomach and other organs in the mediastinum.
Materials and Methods: Thirty patients presented to the University of Kansas with giant paraesophageal hernias. Fifteen patients (50%) were males and 15 were females. The mean age was 65.8 + 14.3 years.
| Symptom | # Patients (%) |
|---|---|
| bloating | 30 (100%) |
| chest pain | 30 (100%) |
| postprandial discomfort | 30 (100%) |
| GERD | 15 (50%) |
| recurrent pneumonias | 1 (3.3) |
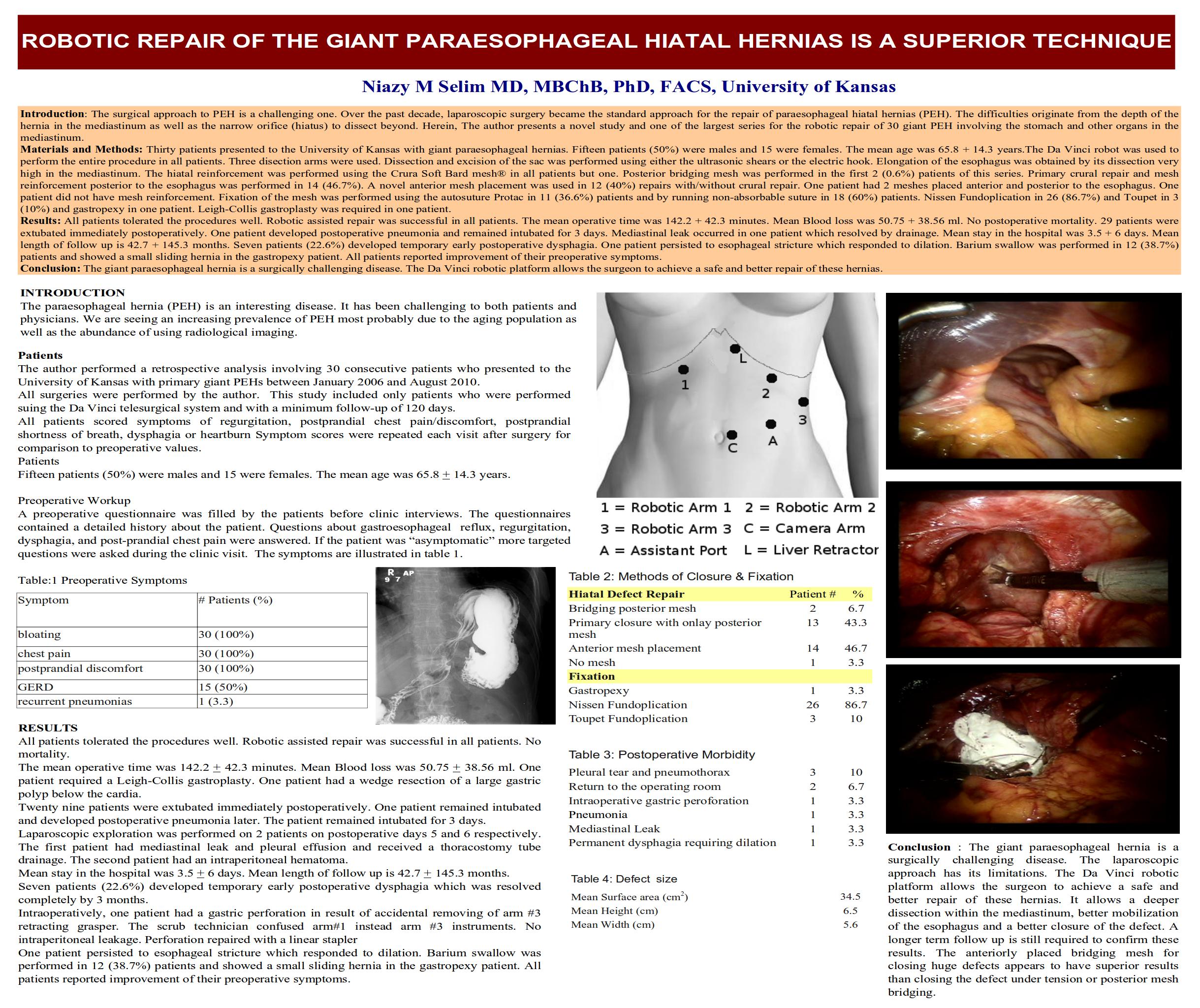
The Da Vinci robot was used to perform the entire procedure in all patients. Three disection arms were used. Dissection and excision of the sac was performed using either the ultrasonic shears or the electric hook. Elongation of the esophagus was obtained by its dissection very high in the mediastinum.
The hiatal reinforcement was performed using the Crura Soft Bard mesh® in all patients. Posterior bridging mesh was performed in the first 2 (0.6%) patients of this series. Primary crural repair and mesh reinforcement posterior to the esophagus was performed in 14 (46.7%). A novel anterior mesh placement was used in 12 (40%) repairs with/without crural repair. One patient had 2 meshes placed anterior and posterior to the esophagus. One patient did not have mesh reinforcement. Nissen Fundoplication in 27 (90%) and Toupet in 3 (0.1%) and gastropexy one in patient. Leigh-Collis gastroplasty was required in one patient.. Fixation of the mesh was performed using the autosuture Protac in 11 (36.6%) patients and by running non-absorbable suture in 18 (60%) patients. Nissen Fundoplication in 26 (86.7%) and Toupet in 3 (10%) and gastropexy in one patient. Leigh-Collis gastroplasty was required in one patient.
Results: All patients tolerated the procedures well. Robotic assisted repair was successful in all patients. The mean operative time was 142.2 + 42.3 minutes. Mean Blood loss was 50.75 + 38.56 ml. No postoperative mortality. 29 patients were extubated immediately postoperatively. One patient developed postoperative pneumonia and remained intubated for 3 days. Mediastinal leak occurred in one patient which resolved by drainage.
Mean stay in the hospital was 3.5 + 6 days. Mean length of follow up is 42.7 + 145.3 months. Seven patients (22.6%) developed temporary early postoperative dysphagia. One patient persisted to esophageal stricture which responded to dilation. Barium swallow was performed in 12 (38.7%) patients and showed a small sliding hernia in the gastropexy patient. All patients reported improvement of their preoperative symptoms.
Conclusion: The giant paraesophageal hernia is a surgically challenging disease. The Da Vinci robotic platform allows the surgeon to achieve a safe and better repair of these hernias.
Session: Poster
Program Number: P499
View Poster
{kind=link}