David Calatayud, MD PhD, Stefano D’ugo, MD, Francesco Coratti, MD, Paolo Raimondi, MD, Federico Gheza, MD, Mario Masrur, MD, Enrique F Elli, MD, Francesco M Bianco, MD, Subashini Ayloo, MD, Pier C Giulianotti, MD FACS. University of Illinois at Chicago Medical Center
INTRODUCTION:
Open surgery is the standard approach for major liver resections. Laparoscopic approach is limited to few hepatic transections. Robotic surgery allows the surgeon to perform complex procedures in the liver, including major resections. This study presents a series of major liver resections performed by the robotic approach, focusing in the intraoperative data concerning the technical surgical aspects, as well as the hemodynamic management.
METHODS AND PROCEDURES:
This study is a single-surgeon series, which included all major hepatic resections performed by robotic approach. Major liver resection is defined by a resection of 3 or more liver segments.We have analyzed intraoperative surgical aspects, as the devices used for the liver transection, or the need of Pringle maneuver. The intraoperative anesthetic management of the hemodynamic status of the patient has been evaluated, focusing on the central venous pressure (CVP) during the transection, the main blood pressure, and the resulting blood loss and requirements for transfusion. The statistical analysis is performed by the IBM SPSS Statistics™ software version 19.
RESULTS:
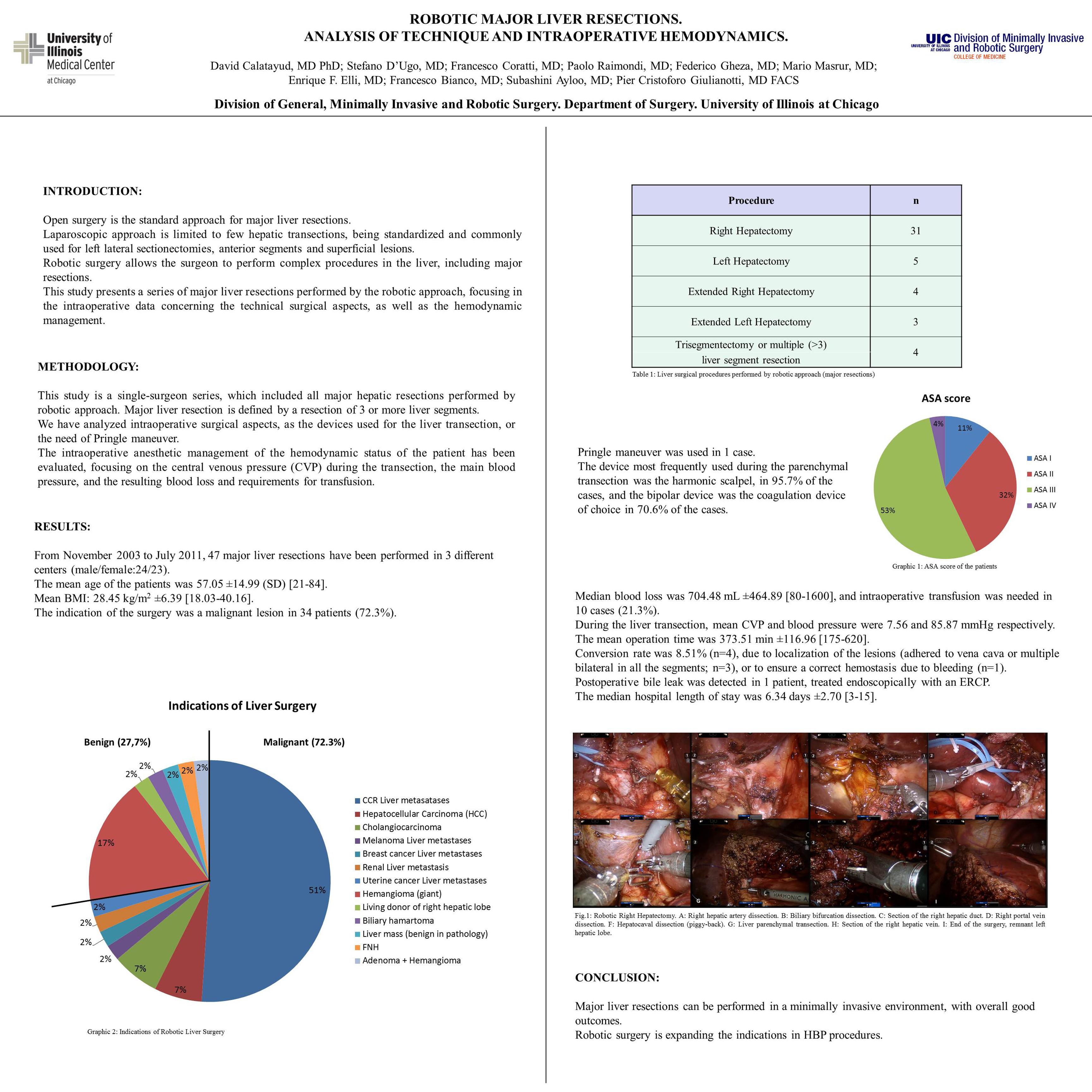
From November 2003 to July 2011, 47 major liver resections have been performed in 3 different centers (male/female: 24/23). The mean age of the patients was 57.01 ±14.98 (SD), with a mean BMI of 27.63 kg/m2 ±6.8. The indication of the surgery was a malignant lesion in 34 patients (72.3%). Procedures were: Right hepatectomy (n=31), left hepatectomy (n=5), extended right hepatectomy (n=4), extended left hepatectomy (n= 3), trisegmentectomy or multiple (>3) liver segment resection (n= 4). Pringle maneuver was used in 1 case. The device most frequently used during the parenchymal transection was the harmonic scalpel, in 95.7% of the cases, and the bipolar device was the coagulation device of choice in 70.6% of the cases. Median blood loss was 600 mL, and intraoperative transfusion was needed in 9 cases (19.1%). During the liver transection, mean CVP and blood pressure were 7.75 and 81.95 mmHg respectively. The mean operation time was 391 min ±137. Conversion rate was 12.8% (n=6). Postoperative bile leak was detected in 1 patient, treated endoscopically with an ERCP. The median hospital length of stay was 6 days ±4.34.
CONCLUSION:
Robot assisted major liver resections seem to be feasible and to have good outcomes. Morbility and tranfusion rate are low. Technical details are discussed . The robotic technology could expand the role of the minimally invasive approach in hepatobiliary surgery.
Session Number: Poster – Poster Presentations
Program Number: P395
View Poster