Joseph L Frenkel, MD, Anthony P D’Andrea, MMS, John H Marks, MD. Lankenau Hospital and Institute for Medical Research, Wynnewood, Pennsylvania
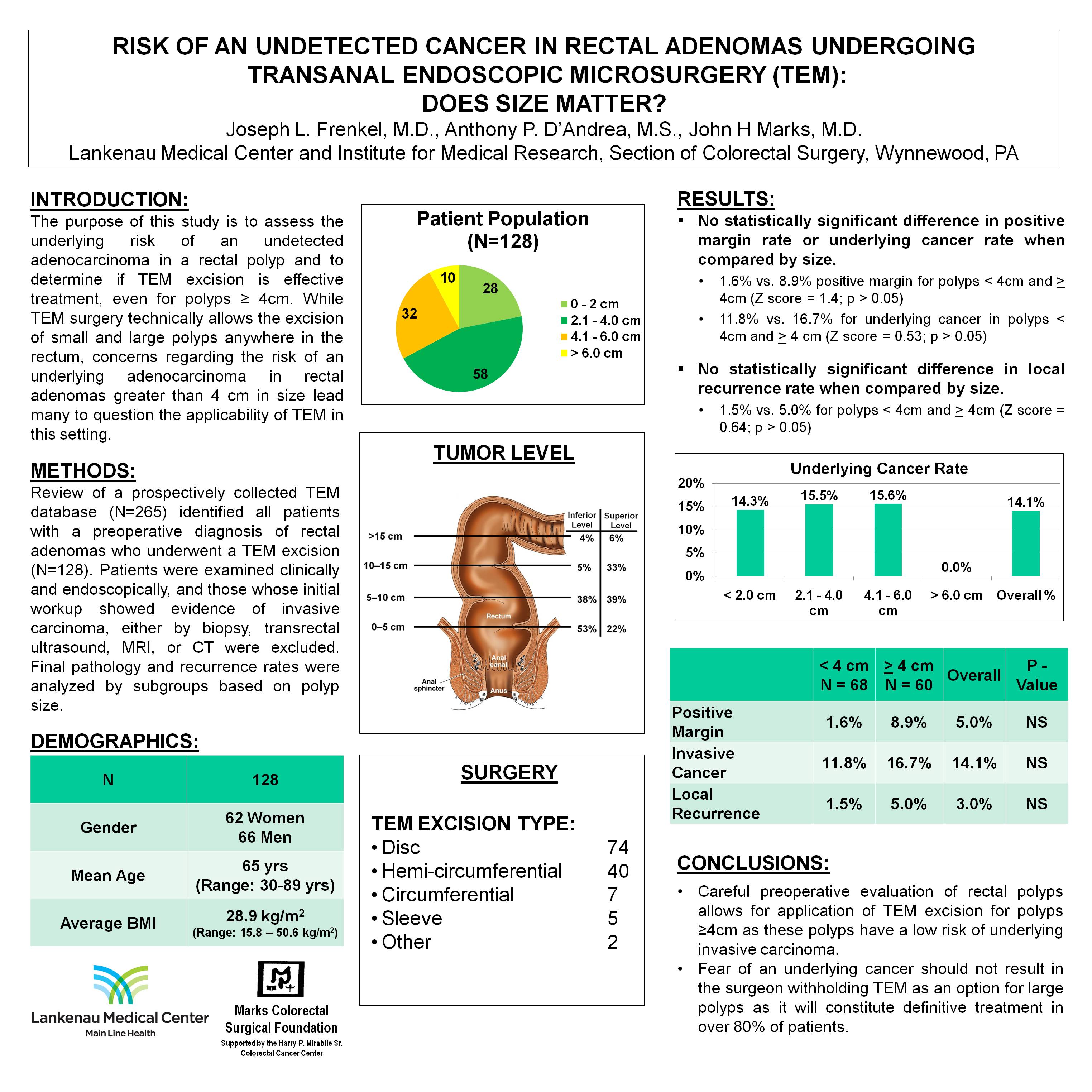
INTRODUCTION: The purpose of this study is to assess the underlying risk of an undetected adenocarcinoma in a polyp and to determine if TEM excision is effective treatment, even for polyps ≥ 4cm. While TEM surgery technically allows the excision of small and large polyps anywhere in the rectum, concerns regarding the risk of an underlying adenocarcinoma in rectal adenomas greater than 4 cm in size lead many to question the applicability of TEM in this setting.
METHODS AND PROCEDURES: Review of a prospectively collected TEM database (N=265) identified all patients with a preoperative diagnosis of rectal adenomas who underwent a TEM excision (N=128). Patients were examined clinically and endoscopically, and those whose initial workup showed evidence of invasive carcinoma, either by biopsy, transrectal ultrasound, MRI, or CT were excluded. Patient outcomes were analyzed by subgroups based on polyp size: 0-2 cm (N=28), 2.1-4 cm (N=58), 4.1-6.0 cm (N=32), and >6.0 cm (N=10); < 4 cm (N=68) vs ≥ 4cm (N=60) regarding final pathology after TEM excision and local recurrence rates (LR).
RESULTS: There were 62 women and 66 men with average age of 65 years (30-89 years). Excisions were as follows: submucosal 40, full thickness 80, not available (NA) 2. There were 5 sleeve, 7 circumferential, 74 disc, and 40 hemi-circumferential excisions. Overall the positive margin rate was 5.0%; 1.6% in the < 4cm group vs 8.9% in the >4 cm group (z score=1.4; p > 0.05). The overall underlying cancer rate was 14.1% with the following rates by size (cm): ≤2cm = 14.3%; 2.1-4.0 cm = 15.5%; 4.1-6.0cm = 15.6%; >6cm = 0. Cancer rate in polyps <4.0cm = 11.8% and ≥4.0cm = 16.7%. (z score – 0.53; p>0.05). With a mean follow up of 25.9 months (1-134 mos), overall local recurrence rate was 3%. LR was 1.5% in the <4cm group, 5% in the ≥4cm group (z score = 0.64, p>0.05).
CONCLUSION: Careful evaluation of polyps while maintaining a high suspicion of cancer allows the application of TEM to excise polyps ≥ 4cm with a low risk of discovering an unsuspected cancer and low LR rates. This data supports the use of TEM to excise both large and small adenomas with excellent outcomes and a reasonable cancer risk. Fear of an underlying cancer shouldn’t result in the surgeon withholding TEM as an option for large polyps as it will constitute definitive treatment in over 80% of patients.
Session: Poster
Program Number: P163
View Poster
{kind=link}