Morimasa Tomikawa, MD PhD FACS, Tomohiko Akahoshi, MD PhD, Yoshihiro Nagao, MD PhD, Makoto Hashizume, MD PhD FACS. Department of Advanced Medicine and Innovative Technology, Kyushu University Hospital
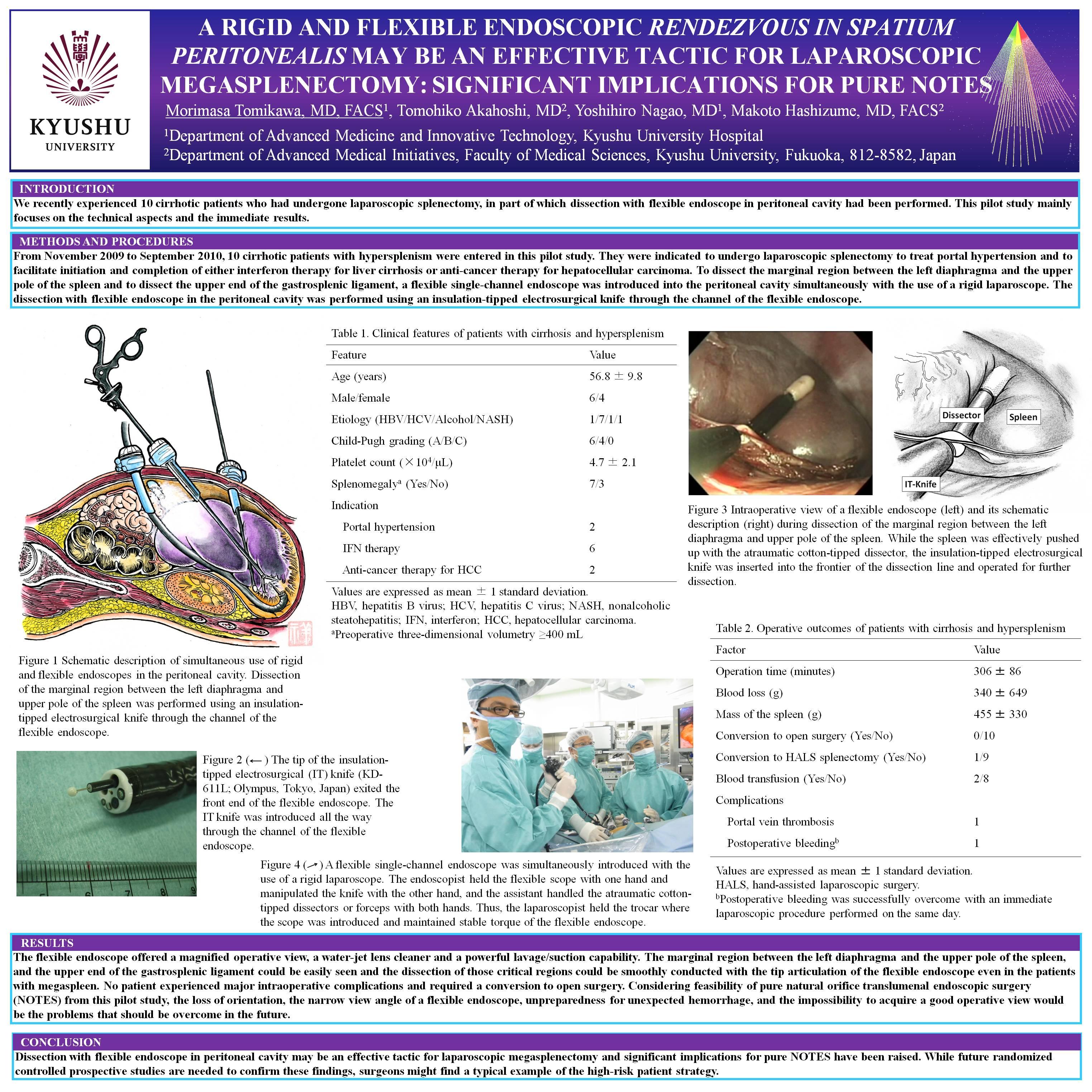
INTRODUCTION: We recently experienced 10 cirrhotic patients who had undergone laparoscopic splenectomy, in part of which dissection with flexible endoscope in peritoneal cavity had been performed. This pilot study mainly focuses on the technical aspects and the immediate results.
METHODS AND PROCEDURES: From November 2009 to September 2010, 10 cirrhotic patients with hypersplenism were entered in this pilot study. They were indicated to undergo laparoscopic splenectomy to treat portal hypertension and to facilitate initiation and completion of either interferon therapy for liver cirrhosis or anti-cancer therapy for hepatocellular carcinoma. To dissect the marginal region between the left diaphragma and the upper pole of the spleen and to dissect the upper end of the gastrosplenic ligament, a flexible single-channel endoscope was introduced into the peritoneal cavity simultaneously with the use of a rigid laparoscope. The dissection with flexible endoscope in the peritoneal cavity was performed using an insulation-tipped electrosurgical knife through the channel of the flexible endoscope.
RESULTS: The flexible endoscope offered a magnified operative view, a water-jet lens cleaner and a powerful lavage/suction capability. The marginal region between the left diaphragma and the upper pole of the spleen, and the upper end of the gastrosplenic ligament could be easily seen and the dissection of those critical regions could be smoothly conducted with the tip articulation of the flexible endoscope even in the patients with megaspleen. No patient experienced major intraoperative complications and required a conversion to open surgery. Considering feasibility of pure natural orifice translumenal endoscopic surgery (NOTES) from this pilot study, the loss of orientation, the narrow view angle of a flexible endoscope, unpreparedness for unexpected hemorrhage, and the impossibility to acquire a good operative view would be the problems that should be overcome in the future.
CONCLUSION: Dissection with flexible endoscope in peritoneal cavity may be an effective tactic for laparoscopic megasplenectomy and significant implications for pure NOTES have been raised. While future randomized controlled prospective studies are needed to confirm these findings, surgeons might find a typical example of the high-risk patient strategy.
Session Number: Poster – Poster Presentations
Program Number: P514
View Poster