Jose G Mejias, MD, Pierina B Rosales, MD, Hector Almau, MD, Rafael De La Fuente, MD, Naydeli Garcia, MD, Carlos Bravo, MD. Clinica Briceno Rossi
PURE NOTES: TRANSVAGINAL TUBAL STERILIZATION WITH FLEXIBLE ENDOSCOPE José Mejías, Pierina Rosales, Hector Almau, Rafael de la Fuente, Naydeli García, Carlos Bravo. Caracas, Venezuela
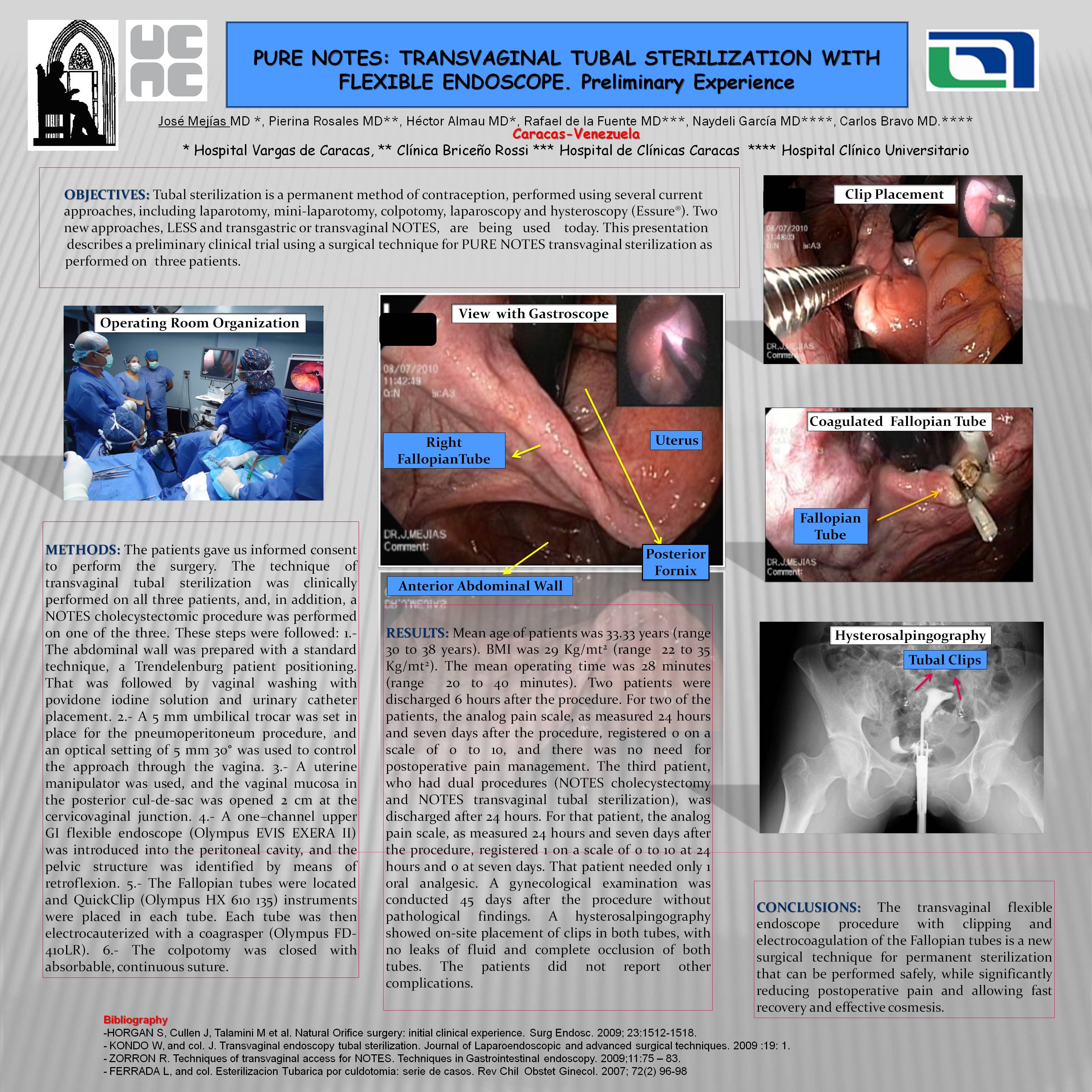
OBJECTIVES: Tubal sterilization is a permanent method of contraception, performed using several current approaches, including laparotomy, mini-laparotomy, colpotomy, laparoscopy and hysteroscopy (Essure®). Two new approaches, LESS and transgastric or transvaginal NOTES, are being used today. This presentation describes a preliminary clinical trial using a surgical technique for PURE NOTES transvaginal sterilization as performed on three patients.
METHODS: The patients gave us informed consent to perform the surgery. The technique of transvaginal tubal sterilization was clinically performed on all three patients, and, in addition, a NOTES cholecystectomic procedure was performed on one of the three. These steps were followed: 1.- The abdominal wall was prepared with a standard technique, a Trendelenburg patient positioning. That was followed by vaginal washing with povidone iodine solution and urinary catheter placement. 2.- A 5 mm umbilical trocar was set in place for the pneumoperitoneum procedure, and an optical setting of 5 mm 30° was used to control the approach through the vagina. 3.- A uterine manipulator was used, and the vaginal mucosa in the posterior cul-de-sac was opened 2 cm at the cervicovaginal junction. 4.- A one–channel upper GI flexible endoscope (Olympus EVIS EXERA II) was introduced into the peritoneal cavity, and the pelvic structure was identified by means of retroflexion. 5.- The Fallopian tubes were located and QuickClip (Olympus HX 610 135) instruments were placed in each tube. Each tube was then electrocauterized with a coagrasper (Olympus FD-410LR). 6.- The colpotomy was closed with absorbable, continuous suture.
RESULTS: Mean age of patients was 33.33 years (range 30 to 38 years). BMI was 29 Kg/mt2 (range 22 to 35 Kg/mt2). The mean operating time was 28 minutes (range 20 to 40 minutes). Two patients were discharged 6 hours after the procedure. For two of the patients, the analog pain scale, as measured 24 hours and seven days after the procedure, registered 0 on a scale of 0 to 10, and there was no need for postoperative pain management. The third patient, who had dual procedures (NOTES cholecystectomy and NOTES transvaginal tubal sterilization), was discharged after 24 hours. For that patient, the analog pain scale, as measured 24 hours and seven days after the procedure, registered 1 on a scale of 0 to 10 at 24 hours and 0 at seven days. That patient needed only 1 oral analgesic. A gynecological examination was conducted 45 days after the procedure without pathological findings. A hysterosalpingography showed on-site placement of clips in both tubes, with no leaks of fluid and complete occlusion of both tubes. The patients did not report other complications.
CONCLUSIONS: The transvaginal flexible endoscope procedure with clipping and electrocoagulation of the Fallopian tubes is a new surgical technique for permanent sterilization that can be performed safely, while significantly reducing postoperative pain and allowing fast recovery and effective cosmesis.
Session: Emerging Technology Poster
Program Number: ETP059
View Poster
{kind=link}