Toni Beninato, MD, David A Nissan, BS, Filippo Filicori, MD, David A Kleiman, MD, Elliot Servais, MD, Thomas J Fahey Iii, MD, Rasa Zarnegar, MD. New York Presbyterian Hospital – Weill Cornell Medical College
Introduction: The objective was to compare surgical outcomes between obese (BMI >30) and non-obese (BMI<30) patients after single-incision laparoscopic cholecystectomy (SILC). A number of observational studies, case series, case controls, and most recently randomized controlled trials have suggested that SILC is a feasible alternative to conventional laparoscopic cholecystectomy. Few articles have investigated the use of SILC on obese patients, and most studies have specifically excluded patients with high BMIs.
Methods and Procedures: This is a prospective study of 72 consecutive patients that underwent SILC by a single surgeon at a tertiary referral center in 2010 and 2011. There were no exclusion criteria. Endpoints included operative time, estimated blood loss, and percent conversion to conventional laparoscopic cholecystectomy. Complication rates were also evaluated. Statistical analysis was done with Student’s t-test or Mann-Whitney U test, where appropriate.
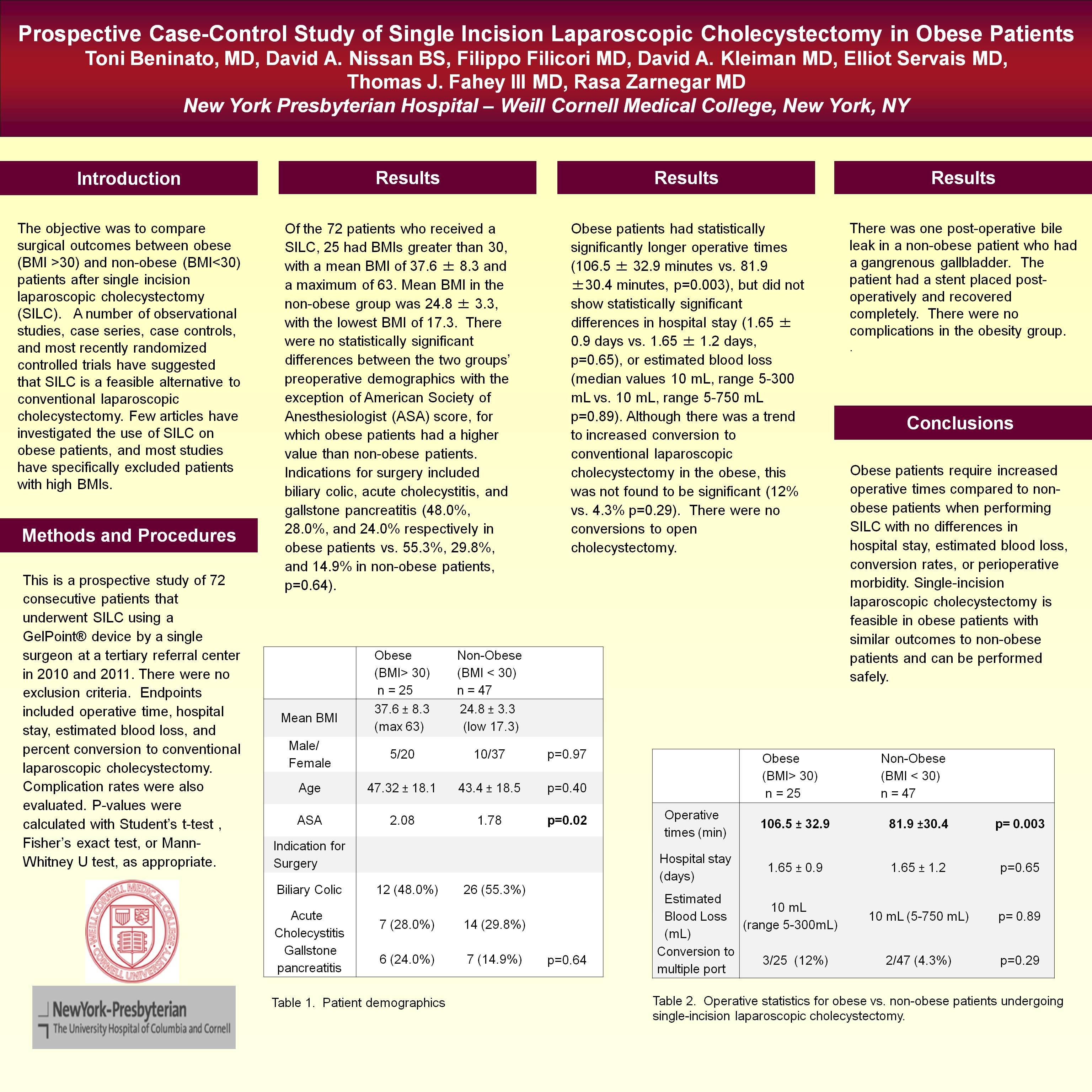
Results: Of the 72 patients who received a SILC, 25 had BMIs greater than 30, with a mean BMI of 37.6 ± 8.3 and a maximum of 63. Mean BMI in non-obese group was 24.8 ± 3.3, with the lowest BMI of 17.3. There were no statistically significant differences between the two groups’ preoperative demographics. Indications for surgery included biliary colic, acute cholecystitis, and gallstone pancreatitis (44.0%, 28.0%, and 24.0% respectively in obese patients vs. 51.1%, 29.8%, and 14.9% in non-obese patients, p=0.52). Obese patients had statistically significantly longer operative times (106.5 ± 32.9 minutes vs. 81.9 ±30.4 minutes, p=0.003), but did not show statistically significant differences in hospital stay (1.65 ± 0.9 days vs. 1.65 ± 1.2 days, p=0.65) or estimated blood loss (median values 10 mL, range 5-300 mL vs. 10 mL, range 5-750 mL p=0.89). Although there was a trend to increased conversion to conventional laparoscopic cholecystectomy in the obese, this was also not found to be significant (12% vs. 4.3% p=0.29). There were no conversions to open cholecystectomy. There was one post-operative bile leak in a non-obese patient with a gangrenous gallbladder. The patient had a stent placed post-operatively and recovered completely. There were no complications in the obesity group.
Conclusions: Obese patients require statistically significantly increased operative times compared to non-obese patients when performing SILC. There were no statistically significant differences in hospital stay, estimated blood loss, conversion rates, or perioperative morbidity. Single-incision laparoscopic cholecystectomy is feasible in obese patients with similar outcomes to non-obese patients and can be performed safely.
| Obese (BMI> 30) n = 25 |
Non-Obese (BMI < 30) n = 47 |
||
|---|---|---|---|
| Indication for Surgery | |||
| Biliary Colic | 12 (48.0%) | 26 (55.3%) | |
| Acute Cholecystitis | 7 (28.0%) | 14 (29.8%) | p=0.52 |
| Gallstone pancreatitis | 6 (24.0%) | 7 (14.9%) | |
| Operative times (min) | 106.5 ± 32.9 | 81.9 ±30.4 | p= 0.003 |
| Hospital stay (days) | 1.65 ± 0.9 | 1.65 ± 1.2 | p=0.65 |
| Estimated Blood Loss (mL) | 10 mL (range 5-300 mL) | 10 mL (5-750 mL) | p= 0.89 |
| Conversion to multiple port | 3/25 (12%) | 2/47 (4.3%) | p=0.29 |
Session Number: Poster – Poster Presentations
Program Number: P599
View Poster