Hiroyuki Fukuda, MD PhD, Kotaro Yoshimura, MD, Hidehito Shibasaki, MD PhD, Takaaki Kaneko, MD PhD, Koya Fushimi, MD PhD, Takashi Senda, MD, Takahito Masuda, MD, Shintaro Kohama, MD, Yangi Mun, MD, Akira Ogata, MD PhD. matsudo city hospital
Objectives:
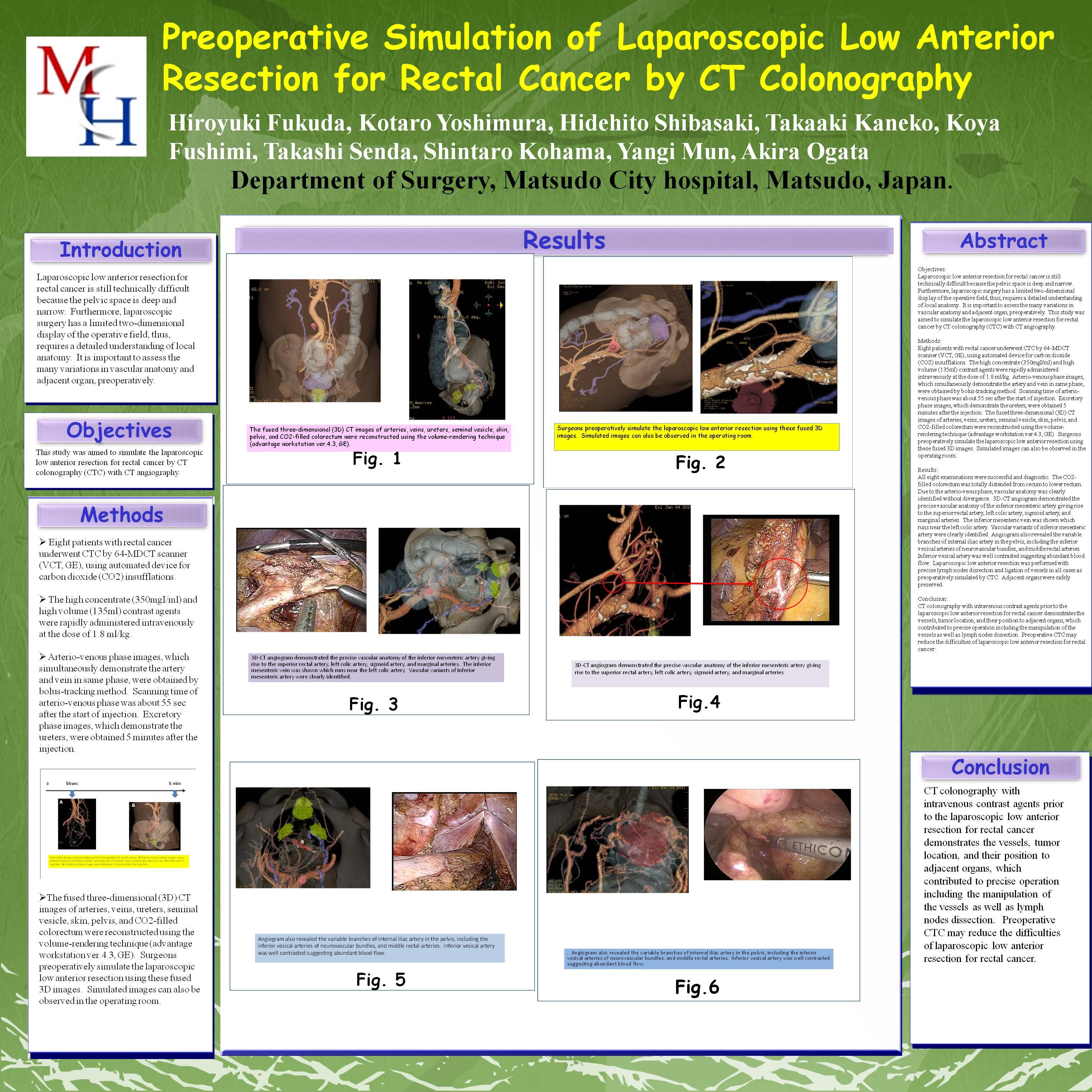
Laparoscopic low anterior resection for rectal cancer is still technically difficult because the pelvic space is deep and narrow. Furthermore, laparoscopic surgery has a limited two-dimensional display of the operative field, thus, requires a detailed understanding of local anatomy. It is important to assess the many variations in vascular anatomy and adjacent organ, preoperatively. This study was aimed to simulate the laparoscopic low anterior resection for rectal cancer by CT colonography (CTC) with CT angiography.
Methods:
Eight patients with rectal cancer underwent CTC by 64-MDCT scanner (VCT, GE), using automated device for carbon dioxide (CO2) insufflations. The high concentrate (350mgI/ml) and high volume (135ml) contrast agents were rapidly administered intravenously at the dose of 1.8 ml/kg. Arterio-venous phase images, which simultaneously demonstrate the artery and vein in same phase, were obtained by bolus-tracking method. Scanning time of arterio-venous phase was about 55 sec after the start of injection. Excretory phase images, which demonstrate the ureters, were obtained 5 minutes after the injection. The fused three-dimensional (3D) CT images of arteries, veins, ureters, seminal vesicle, skin, pelvis, and CO2-filled colorectum were reconstructed using the volume-rendering technique (advantage workstation ver.4.3, GE). Surgeons preoperatively simulate the laparoscopic low anterior resection using these fused 3D images. Simulated images can also be observed in the operating room.
Results:
All eight examinations were successful and diagnostic. The CO2-filled colorectum was totally distended from cecum to lower rectum. Due to the arterio-veous phase, vascular anatomy was clearly identified without divergence. 3D-CT angiogram demonstrated the precise vascular anatomy of the inferior mesenteric artery giving rise to the superior rectal artery, left colic artery, sigmoid artery, and marginal arteries. The inferior mesenteric vein was shown which runs near the left colic artery. Vascular variants of inferior mesenteric artery were clearly identified. Angiogram also revealed the variable branches of internal iliac artery in the pelvis, including the inferior vesical arteries of neurovascular bundles, and middle rectal arteries. Inferior vesical artery was well contrasted suggesting abundant blood flow. Laparoscopic low anterior resection was performed with precise lymph nodes dissection and ligation of vessels in all cases as preoperatively simulated by CTC. Adjacent organs were safely preserved.
Conclusion:
CT colonography with intravenous contrast agents prior to the laparoscopic low anterior resection for rectal cancer demonstrates the vessels, tumor location, and their position to adjacent organs, which contributed to precise operation including the manipulation of the vessels as well as lymph nodes dissection. Preoperative CTC may reduce the difficulties of laparoscopic low anterior resection for rectal cancer.
Session Number: Poster – Poster Presentations
Program Number: P038
View Poster