Thamer Al Abbasi, MB, BCh, BAO, MRCSI, FRCSC, Fady Saleh, MD, MPH, Timothy D Jackson, BSc, MD, MPH, FRCSC, Allan Okrainec, MDCM, MHPE, FRCSC, FACS, Fayez A Quereshy, MD, MBA, FRCSC. University Health Network, University of Toronto, Toronto, Canada.
Introduction: Preoperative repeat endoscopy in colorectal cancer patients has been considered an integral component of surgical planning. It is not without increased cost and morbidity. This study serves to establish the repeat endoscopy rate in patients undergoing surgery for colorectal cancer at a tertiary academic center, to identify significant factors that may influence the decision for preoperative repeat endoscopy, and to evaluate changes in the volume of laparoscopic colectomies over the study period and its relationship with the re-endoscopy rate.
Methods: A retrospective review of 342 consecutive patients undergoing surgical resection for colorectal cancer was performed from January 2008 to December 2011. Descriptive statistics were used to define the patient population and to establish the institutional repeat endoscopy rate. In order to identify factors associated with repeated preoperative endoscopy, univariate and multivariate analysis was used using the chi-square test and logistic regression modeling.
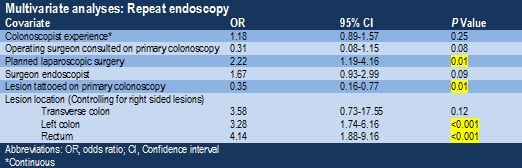
Results: Patients within the two comparison groups had similar demographic profiles. Excluding patients where the primary endoscopist was the operating surgeon, 122 of 299 patients (40.6%) underwent re-endoscopy. The most common reasons for re-endoscopy included tattooing of the lesion in 55 patients (45%), surgical planning in 43 (35.2%), and repeated therapeutic attempts in 11 (9%). A significant delay in operative management was encountered in patients who underwent re-endoscopy (P=0.002). Significant factors associated with repeat endoscopy included left-sided colon cancers (compared to right-sided lesions, P=<0.001), planned laparoscopic procedures (P=0.01), and the absence of a tattoo on the first colonoscopy (P=<0.001). There was also a trend towards a reduction in re-endoscopy if the operating surgeon was consulted at the time of the initial endoscopy (P=0.08). Repeat endoscopy resulted in a significant change in the planned surgical resection in 5 patients (4%). There was a clear trend towards increased laparoscopic procedures over the duration of the study (P=<0.001). Although this did not correlate with an increase in re-endoscopy, it did coincide with a significant increase in pre-operative tattooing at the first colonoscopy (P=<0.001).
Conclusion: In a tertiary academic center, the repeat preoperative endoscopy rate was 40.6%. Re-endoscopy was associated with an initial failure to tattoo the lesion, left-sided colonic neoplasms, and a planned laparoscopic resection. While re-endoscopy has the potential to alter surgical planning, this theoretical advantage may be realized in a select group of patients given that it is a procedure associated with increased cost, potential morbidity, and a delay in definitive therapy. Although the growing trend towards laparoscopic surgery did not yield the expected increase in re-endoscopy rate, it may be explained by an institutional increase in preoperative tattoo localization. Further research is needed to help identify which patients would benefit from repeat endoscopy and where this may be safely omitted.