Abhishek Sundaram, MBBS MPH, Brittany L Willer, MD, Zachary H Torgersen, BA, Arpad Juhasz, MD PhD, Masato Hoshino, MD, Tommy H Lee, MD, Sumeet K Mittal, MD. Division of General Surgery, Creighton University Medical Center
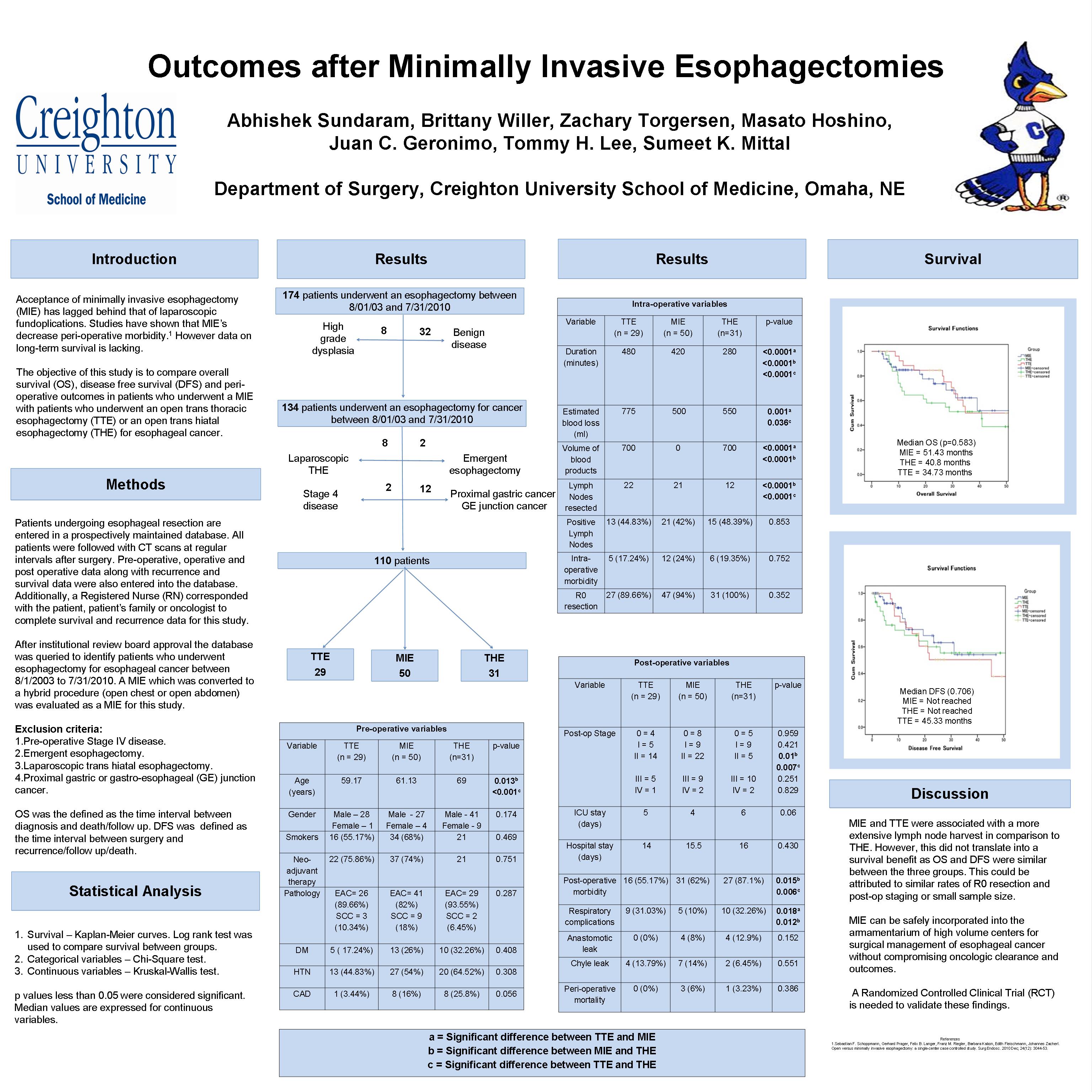
Objective: The objective of this study was to compare overall survival (OS) and disease free survival (DFS) among patients who underwent minimally invasive esophagectomy (MIE), trans thoracic esophagectomy (TTE) or trans hiatal esophagectomy (THE) for esophageal cancer. Studies have demonstrated that MIE improves peri-operative morbidity, however data on long term OS and DFS are lacking.
Methods: A retrospective review of a prospectively maintained database was performed to identify patients who underwent an elective esophagectomy for esophageal cancer at a single institution between 1/1/2003 and 12/31/2008. Non-malignant esophageal pathology, emergent procedures, esophagectomies with an intrathoracic anastomosis, colonic or jejunal interposition grafts were excluded. OS was defined as the interval between diagnosis and follow up or death. DFS was defined as the interval between surgery and recurrence in the form of local recurrence or metastatic disease. Chi-square test was used to compare categorical variables. T-test and Mann-Whitney tests were used to compare continuous variables. Kaplan-Meier survival analysis was used to evaluate OS and DFS. The log rank test was used to compare OS and DFS.
Results: One hundred and thirty three patients underwent esophagectomies during the study period of which 78 patients satisfied the study criteria. Of these 25 underwent a MIE, 22 underwent a TTE and 31 underwent a THE. The three groups were balanced (p>0.05) in terms of neo-adjuvant therapy and co-morbid conditions. There was no significant difference between the three groups in terms of pre-treatment American Joint Committee on Cancer staging (p=0.49), post-operative pathological staging (p=0.76) and number of R0 resections (p=0.28). While there was no difference (p>0.05) in the number of lymph nodes resected between the MIE (median=16) and TTE groups or the MIE and THE groups, the lymph node harvest in the TTE group (median=17) was greater (p=0.009) than the THE group (median=12). There was no difference (p=0.721) between the groups in terms of recurrence. The log rank test on the Kaplan-Meier survival analysis revealed that there was no significant difference (p=0.591) in OS between TTE (median survival=52.6 months), MIE (median survival = 39.73 months) and THE (median survival=29.71 months). Neither was there a significant difference (p=0.639) in DFS between TTE (median DFS=45.33 months), MIE and THE (median DFS has not been reached in both the groups). When TTE and THE were grouped together and compared to MIE, there still was no significant difference (p>0.05) between them in terms of pre-treatment stage, post-operative pathological stage, number of lymph nodes resected, R0 resection, OS and DFS.
Conclusions: MIE provided an equivalent oncologic clearance to TTE and THE, which is reflected by comparable OS and DFS. TTE was associated with a greater lymph node harvest than THE, but was similar to MIE. Longer follow up and randomized controlled trials are needed to validate these findings.
Session: Poster
Program Number: P289
View Poster
{kind=link}