Introduction: NOTES transanal endoscopic rectosigmoid resection was previously demonstrated using the TEM platform (Transanal Endoscopic Microsurgery). However, the length of left colonic mobilization has been limited due to difficulties with instrument reach and tissue manipulation using standard TEM and endoscopic instrumentation. Recently, a novel innovative sterile sigmoid access platform (ISSA, Storz, Tuttlingen, Germany) was developed to allow the insertion of a flexible endoscope through the sigmoid colon into the abdominal cavity via a rigid rotatable curved 18 mm by 310 mm endoscopic trocar overtube. In this study we evaluated whether the ISSA platform, in conjunction with standard TEM, endoscopic and laparoscopic instruments, could facilitate transanal endoscopic rectosigmoid and left colon resection in ten human male and female cadavers.
Methods: The distal rectum was occluded by placing a pursestring suture approximately 4 cm from the anal verge. Starting just distal to the pursestring, full-thickness rectal dissection with total mesorectal excision was performed endoscopically through the TEM platform using standard TEM and laparoscopic instruments. Upon completion of the rectal and mesorectal dissection and entry into the peritoneal cavity, the inferior mesenteric pedicle and rectosigmoid mesentery were divided and the sigmoid and left colon were mobilized until visualization and mobility were restricted. In some cases, further endoscopic dissection was performed using a gastroscope inserted through the TEM platform. Next, the TEM platform was replaced by the ISSA and the trocar overtube was advanced into the abdominal cavity. A gastroscope was then inserted through the overtube and used to mobilize the proximal colon up to the level of the splenic flexure, with tissue retraction provided through the other ISSA ports. Once maximal mobilization of the left colon was achieved, the colon was exteriorized transanally, inspected and measured.
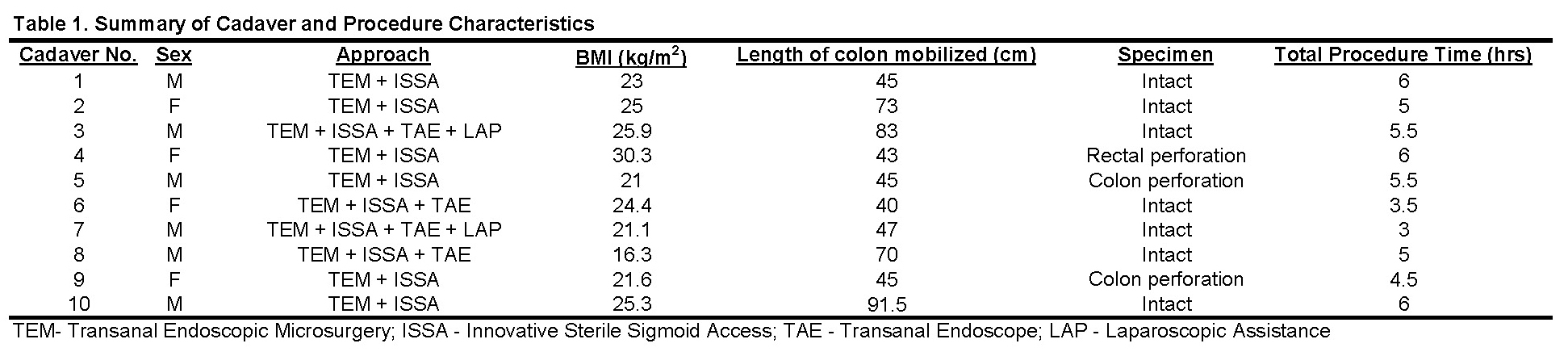
Results: Between November 2010 and August 2011, transanal rectosigmoid and left colon resection was performed using the TEM and ISSA platforms in 6 male and 4 female fresh human cadavers with mean BMI of 24 kg/m2 (range 16.3-30.3). In 4 cadavers, left colonic endoscopic mobilization was first performed using a gastroscope through the TEM platform followed by ISSA. In 2 cadavers, laparoscopic assistance was used for tissue retraction. Mean operative time was 5 hours (range 3-6) and mean specimen length 58.2 cm (range 40-91.5). In 3 cadavers, endoscopic dissection was complicated by colonic or rectal perforation. Results are summarized in Table 1.
Conclusion: NOTES transanal rectosigmoid and left colon resection using the ISSA platform provides ergonomic advantages to standard dissection using the TEM platform and flexible endoscopes. The rigid endoscopic trocar overtube provides additional stability which facilitates the positioning, orientation, tissue manipulation and dissection of the transanal endoscope. The ISSA might help extend the length of rectosigmoid mobilized transanally, and facilitate more proximal colon mobilization during NOTES transanal colorectal procedures.