Rebecca A Levine, MD, Bhani Chawla, MD, Shelli Bergeron, NC, Harry Wasvary, MD. William Beaumont Hospital
INTRODUCTION:
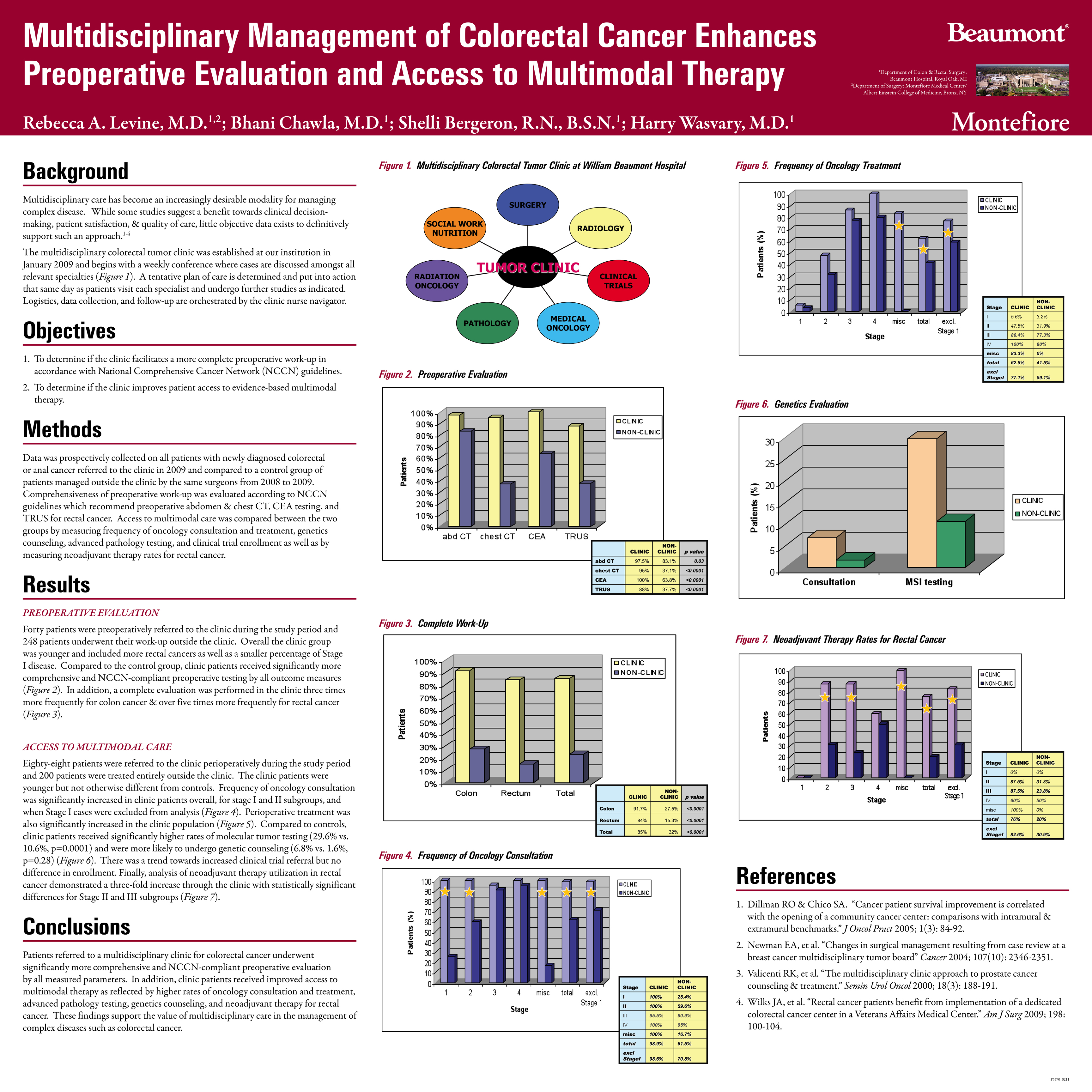
The purpose of our study was to determine the impact of a multidisciplinary clinic on preoperative evaluation and access to multimodal care for patients with colorectal cancer.
METHODS:
Data was prospectively collected on all patients with newly diagnosed colon, rectal, or anal cancer who were referred to the multidisciplinary tumor clinic at our institution from January to December 2009 and compared to a control group of all patients who were managed outside the clinic by the same surgeons from January 2008 to December 2009. The comprehensiveness of preoperative work-up was measured according to NCCN guidelines which require abdomen CT, chest CT, and CEA testing, as well as TRUS for rectal cancer. Access to multimodal therapy was also compared between the clinic & non-clinic patients by measuring frequency of oncology consultation and treatment, genetics consultation, advanced pathology testing, and clinical trial enrollment. In addition, subgroup analysis of neoadjuvant therapy rates in rectal cancer was also performed. Statistical evaluation was completed using Pearson’s Chi-square & Fisher’s exact tests, as well as the student t-test for demographics.
RESULTS:
Two hundred and eighty-eight patients were treated for newly diagnosed colorectal or anal cancer at William Beaumont Hospital from 2008 to 2009. Within this population, forty patients were referred to the clinic preoperatively and forty-eight patients were referred postoperatively. Two hundred patients were never treated in the clinic at all during the study period. In terms of preoperative evaluation, clinic patients underwent significantly more NCCN-compliant testing than patients managed outside the clinic–abdomen CT (97.5% vs. 83.1%, p=0.03), chest CT (95% vs. 37.1%, p<0.0001), CEA testing (100% vs. 63.8%, p<0.0001), and TRUS for rectal cancer (88% vs. 37.7%, p<0.0001). In addition, a complete preoperative work-up was performed in the clinic group over three times more frequently for colon cases and over five times more frequently for rectal cancers when compared to the non-clinic group. Access to multimodal therapy was also significantly enhanced in patients referred to the clinic as measured by frequency of oncology consultation (98.9% vs. 61.5%, p<0.0001) and treatment (62.5% vs. 41.5%, p=0.02), as well as rates of advanced pathology testing (29.6% vs. 10.6%, p=0.0001). Clinical trial enrollment was not different between the two groups but there was a trend towards increased genetics consultation in the clinic population (6.8% vs. 1.6%, p=0.28). Finally, subgroup analysis of rectal cancer patients demonstrated significantly higher rates of neoadjuvant therapy in the clinic group for stage II or greater disease (82.6% vs. 30.9%, p=0.0001), as well as for Stages II & III disease separately (87.5% vs. 31.3%, p=0.03, and 87.5% vs. 23.8%, p=0.003).
CONCLUSIONS:
We found that patients referred to a multidisciplinary clinic for colorectal cancer received significantly more comprehensive preoperative evaluation as well as improved access to multimodal care as indicated by higher rates of oncology consultation and treatment, advanced pathology testing, genetics consultation, and neoadjuvant therapy for rectal cancer. These findings support the value of multidisciplinary care in the management of complex diseases such as colorectal cancer.
Session: Poster
Program Number: P176
View Poster
{kind=link}