David Calatayud, MD PhD, Venkata R Kakarla, MD, Francesco Coratti, MD, Paolo Raimondi, MD, Stefano D’ugo, MD, Luca Milone, MD, Federico Gheza, MD, Mario Masur, MD, Enrique F Elli, MD, Francesco Bianco, MD, Subashini Ayloo, MD, Pier C Giulianotti, MD FACS. University of Illinois at Chicago Medical Center
Background: Laparoscopy is currently the standard approach to cholecystectomy. Large series of robotic assistance have yet to be performed
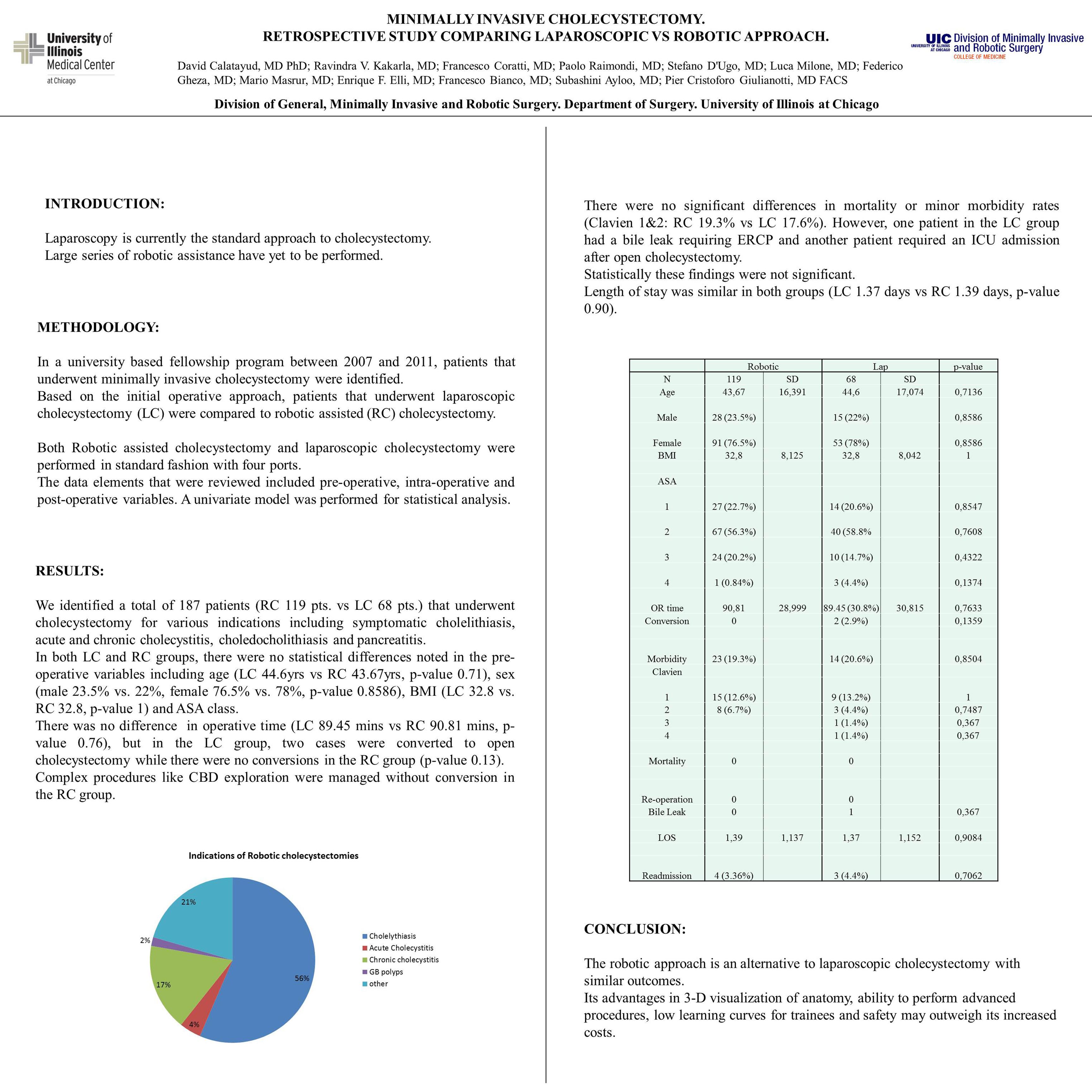
Methods: In a university based fellowship program between 2007 and 2011, patients that underwent minimally invasive cholecystectomy were identified. Based on the initial operative approach, patients that underwent laparoscopic cholecystectomy (LC) were compared to robotic assisted (RC) cholecystectomy. Both Robotic assisted cholecystectomy and laparoscopic cholecystectomy were performed in standard fashion with four ports. The data elements that were reviewed included pre-operative, intra-operative and post-operative variables. A univariate model was performed for statistical analysis.
Results: We identified a total of 187 patients (RC 119 pts. vs LC 68 pts.) that underwent cholecystectomy for various indications including symptomatic cholelithiasis, acute and chronic cholecystitis, choledocholithiasis and pancreatitis. In both LC and RC groups, there were no statistical differences noted in the pre-operative variables including age (LC 44.6yrs vs RC 43.67yrs, p-value 0.71), sex (male 23.5% vs. 22%, female 76.5% vs. 78%, p-value 0.8586), BMI (LC 32.8 vs. RC 32.8, p-value 1) and ASA class. There was no difference in operative time (LC 89.45 mins vs RC 90.81 mins, p-value 0.76), but in the LC group, two cases were converted to open cholecystectomy while there were no conversions in the RC group (p-value 0.13). Complex procedures like CBD exploration were managed without conversion in the RC group. There were no significant differences in mortality or minor morbidity rates (Clavien 1&2: RC 19.3% vs LC 17.6%). However, one patient in the LC group had a bile leak requiring ERCP and another patient required an ICU admission after open cholecystectomy. Statistically these findings were not significant. Length of stay was similar in both groups (LC 1.37 days vs RC 1.39 days, p-value 0.90).
Conclusion: The robotic approach is an alternative to laparoscopic cholecystectomy with similar outcomes. Its advantages in 3-D visualization of anatomy, ability to perform advanced procedures, low learning curves for trainees and safety may outweigh its increased costs.
Session Number: Poster – Poster Presentations
Program Number: P589
View Poster