Albert M Wolthuis, MD, Christel Meuleman, MD, Carla Tomassetti, MD, Thomas D’Hooghe, MD PhD, Steffen Fieuws, PhD, Freddy Penninckx, MD PhD, André D’Hoore, MD PhD. Department of Abdominal Surgery, Leuven University Fertility Centre, Department of Obstetrics and Gynecology, Interuniversity Centre for Biostatistics and Statistical Bioinformatics
Introduction
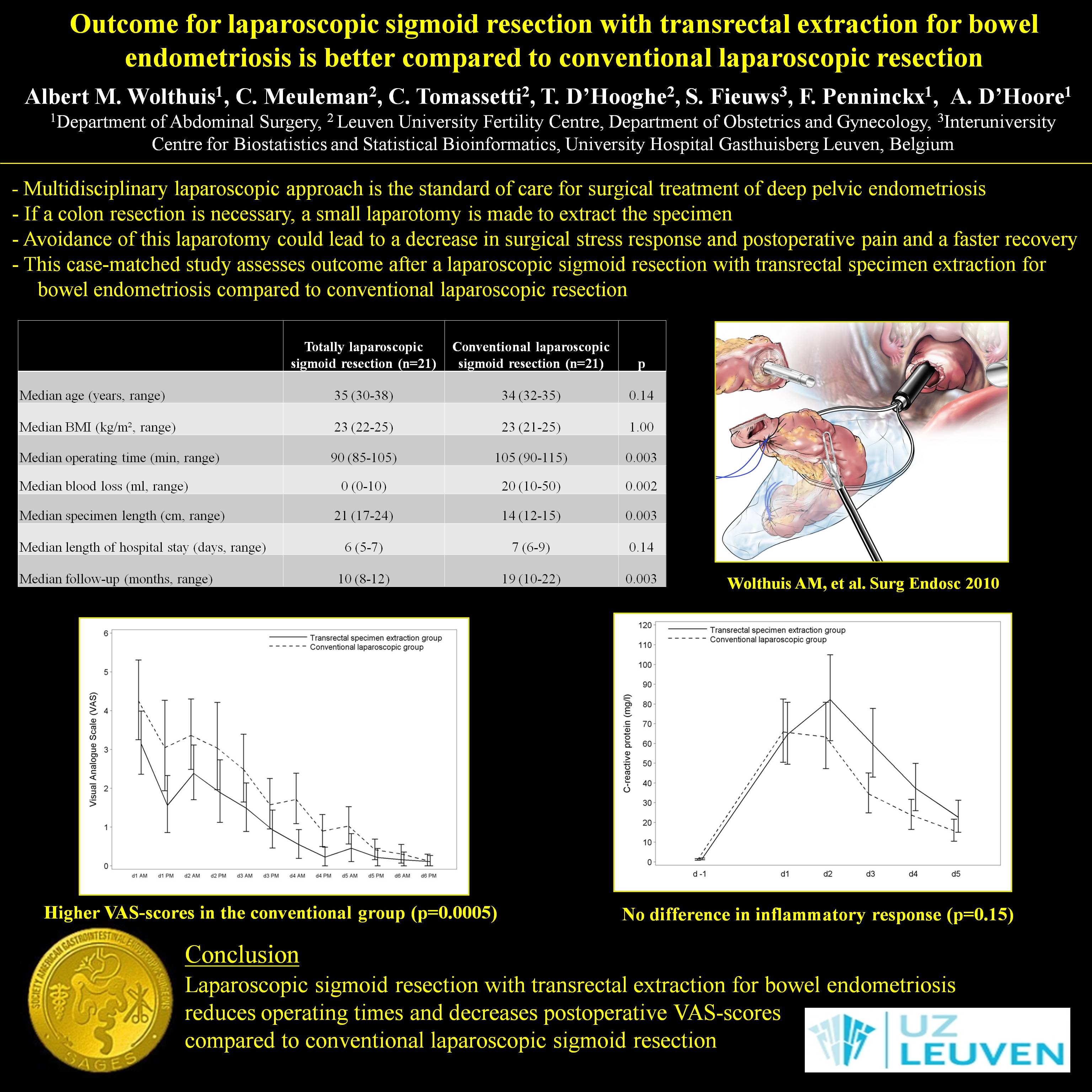
Multidisciplinary laparoscopic treatment is the standard of care for radical treatment of deep infiltrating pelvic endometriosis. If a bowel resection is necessary, a muscle-split or Pfannenstiel incision is made to extract the colon and to create the proximal part of the anastomosis. The avoidance of any laparotomy could lead to a decrease in surgical stress response, a faster return to normal bowel function, a decrease in postoperative pain, less wound complications and incisional hernias. This study assesses postoperative outcome after a laparoscopic sigmoid resection with transrectal specimen extraction for bowel endometriosis.
Patients and methods
Twenty-one patients who underwent elective laparoscopic sigmoid resection with transrectal specimen extraction for bowel endometriosis from September 2009 to September 2010 were matched for age, American Society of Anaesthesiologists class (ASA score) and body mass index (BMI) to a patient who underwent a conventional laparoscopic sigmoid resection. The groups were compared for peri-operative factors, complications, length of hospital stay, postoperative pain using the Visual Analogue Scale (VAS), analgesics consumption and inflammatory response (C-reactive protein).
Results
Patient demographics were similar between treatment groups owing to an adequate matching process. Median operating time was 15 minutes shorter with transrectal specimen extraction (p=0.003). VAS-scores and use of analgesics were significantly higher in the conventional laparoscopic group (p=0.0005). Mean CRP-level was 38% higher in the transrectal specimen extraction group, but not significant (p=0.054). There was no significant difference between increase in CRP in both groups (p=0.15). There were no anastomotic leaks, nor reinterventions in both groups. Median hospital stay was similar in both groups. At follow-up, no wound infections or incisional hernias were observed and none of the patients reported anal dysfunction.
Conclusion
Laparoscopic sigmoid resection with transrectal specimen extraction reduced operating times and decreased postoperative VAS-scores and analgesic requirements compared to conventional laparoscopic sigmoid resection for bowel endometriosis.
Session: Emerging Technology Poster
Program Number: ETP101
View Poster
{kind=link}