Jun Seok Park, MD, Gyu-Seog Choi, MD, Soo Han Jun, MD, Suguru Hasegawa, MD, Yoshiharu Sakai, MD. Department of Surgery, Kyungpook National University Hospital, Department of Surgery, Kyoto University Hospital
Objective: Although there is some evidence of the laparoscopic ISR with CAA, controversy exists because prior conclusions are based on noncomparative study designs, relatively small numbers of cases and only short-term follow-up. This study eas conducted to compare laparoscopic vs. open intersphincteric resection (ISR) with coloanal anastomosis (CAA) for surgical outcome and intermediate oncological outcomes.
Purpose: Although there is some evidence of the laparoscopic ISR with CAA, controversy exists because prior conclusions are based on noncomparative study designs, relatively small numbers of cases and only short-term follow-up.
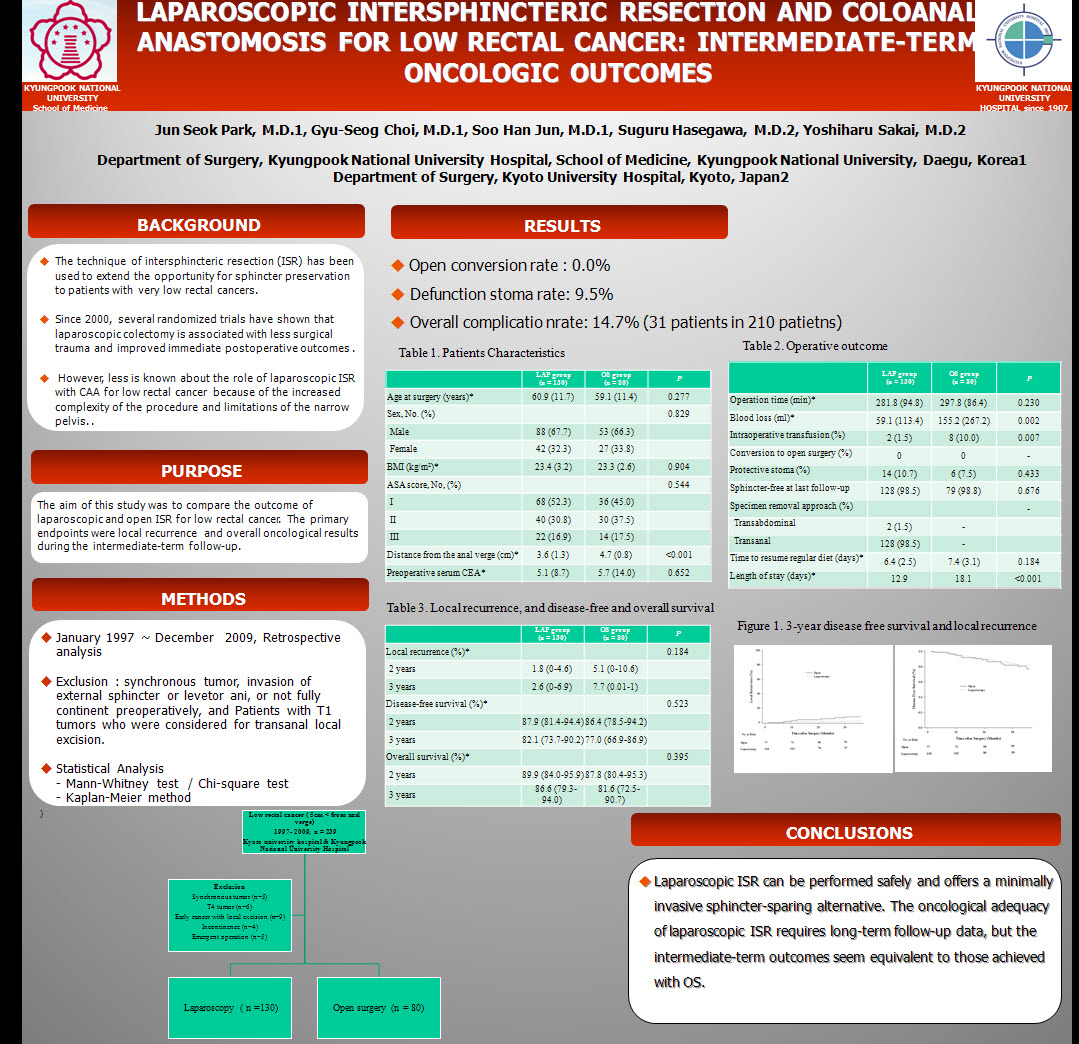
Methods: Two hundred ten consecutive patients with low rectal cancer who underwent curative ISR with CAA between 1997 and 2009 in two institutions were retrospectively evaluated. Patients were classified into an open surgery group (OS, n = 80) and a laparoscopic surgery group (LAP, n = 130). Data include operating time, length of recovery, morbidity, quality of total mesorectal excision, and oncological outcome.
Results: Baseline clinical characteristics and pathological stage was similar in the two groups. In the LAP group, operating time was 16 minutes shorter (P = 0.230) and intraoperative blood loss was significantly lower (P = 0.002). The LAP group had a shorter time to bowel movement (2.6 vs. 3.2 days, P = 0.017) and length of stay (12.9 vs. 18.1 days, P < 0.001). Median follow-up was 30.5 months (interquartile range, 16.0–36.0 months) for the LAP group and 36 months (interquartile range, 26.5–36.0 months) for the OS group. The three-year disease-free survival and local recurrence rates were also similar between the two groups.
Conclusions: Laparoscopic ISR with CAA is safe and effective for patients with low rectal cancer. Midterm oncological outcome after laparoscopic ISR with CAA was comparable to that after conventional approach.
Session: Poster
Program Number: P145
View Poster
{kind=link}