Background: Gastric outlet obstruction (GOO) from abdominal malignancies reduces the quality of life of the patients and needs gastrojejunostomy or endoscopic stenting (ES). Patients who are indicated to this kind of management tend to have advanced diseases. Therefore, safe and less invasive treatment with early recovery should be considered. Laparoscopic gastrojejunostomy (LGJ) is currently feasible and standard palliation for this condition. Here we show the surgical methods and clinical outcome of LGJ in our institution.
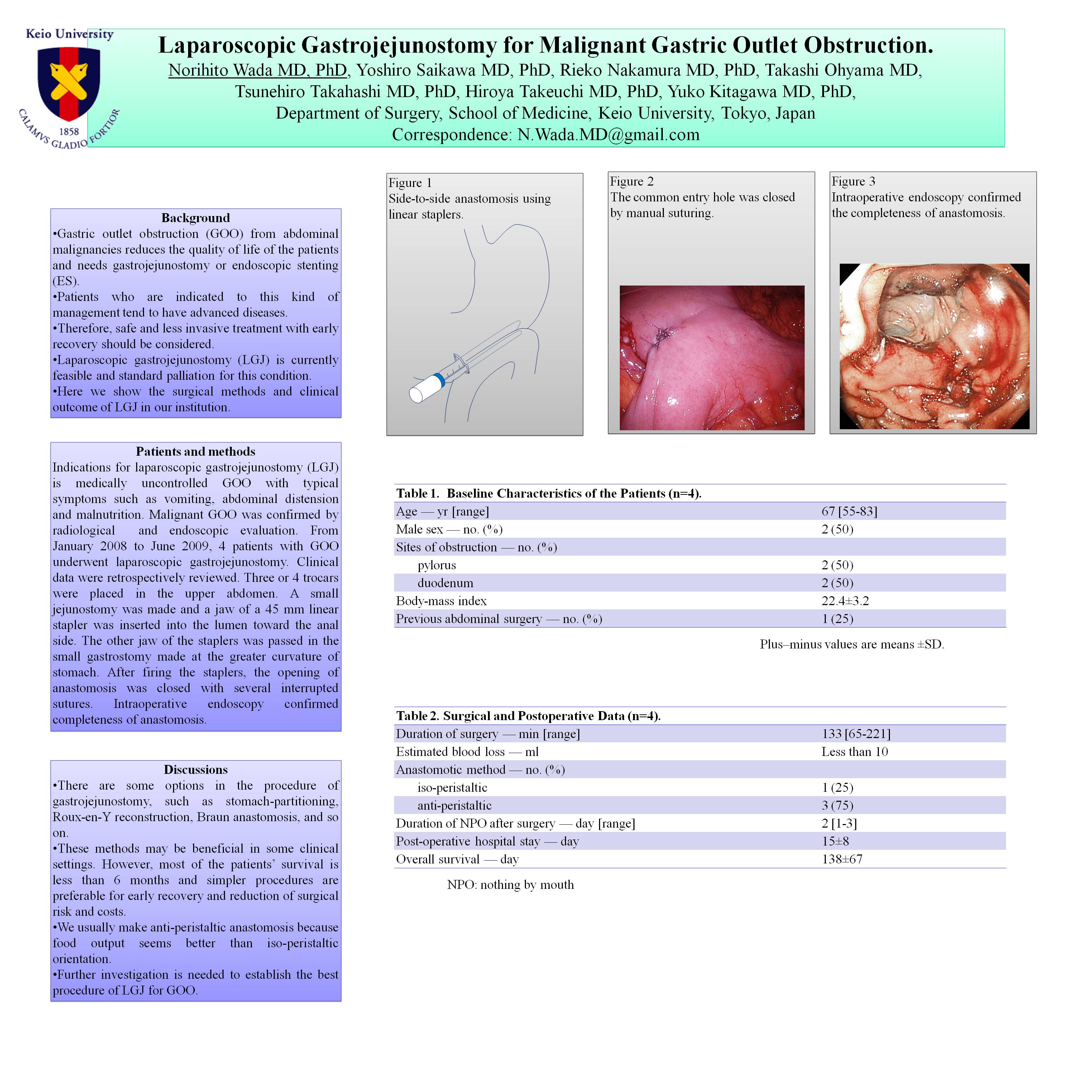
Patients and methods: Indications for laparoscopic gastrojejunostomy (LGJ) is medically uncontrolled GOO with typical symptoms such as vomiting, abdominal distension and malnutrition. Malignant GOO was confirmed by radiological and endoscopic evaluation. From January 2008 to June 2009, 4 patients with GOO underwent laparoscopic gastrojejunostomy. Clinical data were retrospectively reviewed. Three or 4 trocars were placed in the upper abdomen. A small jejunostomy was made and a jaw of a 45 mm linear stapler was inserted into the lumen toward the anal side. The other jaw of the staplers was passed in the small gastrostomy made at the greater curvature of stomach. After firing the staplers, the opening of anastomosis was closed with several interrupted sutures. Intraoperative endoscopy confirmed completeness of anastomosis. Results: Mean age of the patients was 67 [55-83] years old. Half of the patients were female. The sites of obstruction were pylorus (2 patients) and duodenum (2 patients). Surgery time ranges from 1:05 to 3:41. In one case, Braun’s side-to-side anastomosis has been added. No surgical complications and conversion to open surgery were observed. All the patients could start liquid meal in two days, but had died from original malignancies within 6 months.
Discussions: There are some options in the procedure of gastrojejunostomy, such as stomach-partitioning, Roux-en-Y reconstruction, Braun anastomosis, and so on. These methods may be beneficial in some clinical settings. However, most of the patients’ survival is less than 6 months and simpler procedures are preferable for early recovery and reduction of surgical risk and costs. We usually make anti-peristaltic anastomosis because food output seems better than iso-peristaltic orientation. Further investigation is needed to establish the best procedure of LGJ for GOO.
Session: Poster
Program Number: P328

{kind=link}