Emilia Krol, MD, Keith Zuccala, MD, Laura Choi, MD. Danbury Hospital
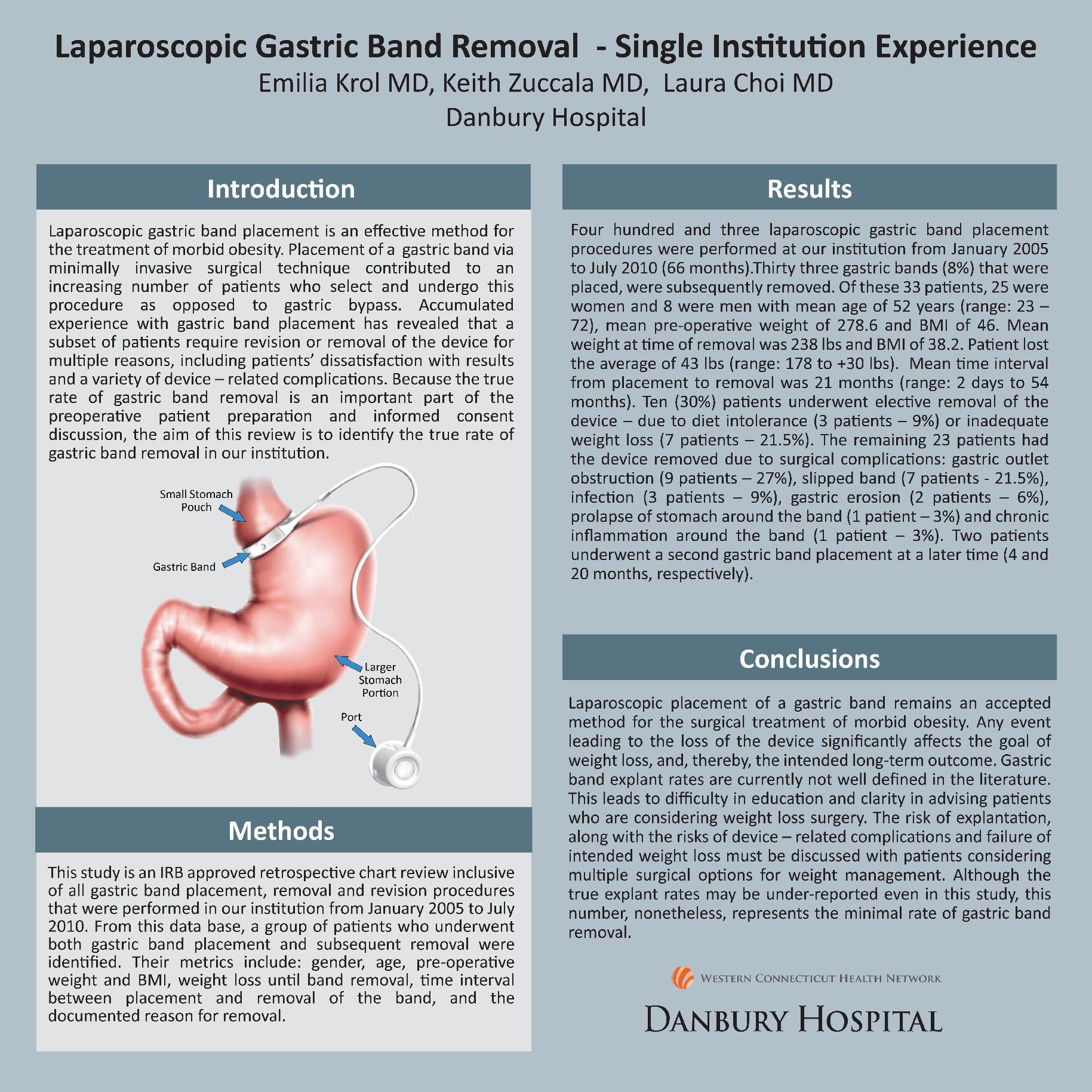
Introduction: Laparoscopic gastric band placement is an effective method for the treatment of morbid obesity. Placement of a gastric band via minimally invasive surgical technique contributed to an increasing number of patients who select and undergo this procedure as opposed to gastric bypass. Accumulated experience with gastric band placement has revealed that a subset of patients require revision or removal of the device for multiple reasons, including patients’ dissatisfaction with results and a variety of device – related complications. Because the true rate of gastric band removal is an important part of the preoperative patient preparation and informed consent discussion, the aim of this review is to identify the true rate of gastric band removal in our institution.
Methods: This study is an IRB approved retrospective chart review inclusive of all gastric band placement, removal and revision procedures that were performed in our institution from January 2005 to July 2010. From this data base, a group of patients who underwent both gastric band placement and subsequent removal were identified. Their metrics include: gender, age, pre-operative weight and BMI, weight loss until band removal, time interval between placement and removal of the band, and the documented reason for removal.
Results: Four hundred and three laparoscopic gastric band placement procedures were performed at our institution from January 2005 to July 2010 (66 months).Thirty three gastric bands (8%) that were placed, were subsequently removed. Of these 33 patients, 25 were women and 8 were men with mean age of 52 years (range: 23 – 72), mean pre-operative weight of 278.6 and BMI of 46. Mean weight at time of removal was 238 lbs and BMI of 38.2. Patient lost the average of 43 lbs (range: 178 to +30 lbs). Mean time interval from placement to removal was 21 months (range: 2 days to 54 months). Ten (30%) patients underwent elective removal of the device – due to diet intolerance (3 patients – 9%) or inadequate weight loss (7 patients – 21.5%). The remaining 23 patients had the device removed due to surgical complications: slipped band (17 patients – 51.5%), infection (3 patients – 9%), gastric erosion (2 patients – 6%), and chronic inflammation around the band (1 patient – 3%). Two patients underwent a second gastric band placement at a later time (4 and 20 months, respectively).
Conclusions: Laparoscopic placement of a gastric band remains an accepted method for the surgical treatment of morbid obesity. Any event leading to the loss of the device significantly affects the goal of weight loss, and, thereby, the intended long-term outcome. Gastric band explant rates are currently not well defined in the literature. This leads to difficulty in education and lack of clarity in advising patients who are considering weight loss surgery. The risk of explantation, along with the risks of device – related complications and failure of intended weight loss must be discussed with patients who consider multiple surgical options for weight management.
Session Number: Poster – Poster Presentations
Program Number: P477
View Poster