Muhammad Asad Khan, MD, Roman Grinberg, MD, Stelin Johnson, RPAC, John N Afthinos, MD, Karen E Gibbs, MD. Staten Island University Hospital
OBJECTIVE:
Laparoscopic cholecystectomy has been the accepted standard of care for the treatment of acute cholecystitis for over a decade. There is ongoing debate whether it is safe in the super morbidly obese patient with BMI ≥ 50 kg/m2. The current study compared the outcomes of super-obese (BMI ≥ 50 kg/m2) patients undergoing open vs. laparoscopic cholecystectomy.
METHODS:
We obtained data from the American College of Surgeons’ National Surgical Quality Improvement Program (NSQIP) on 1062 super-obese patients with a BMI ≥ 50 kg/m2 who underwent open and laparoscopic cholecystectomy between 2007 and 2009. The parameters analyzed included age, gender, co-morbid conditions, American Society of Anesthesiologists classification score, operative time, postoperative complications, re-operation, length of hospital stay and mortality.
RESULTS:
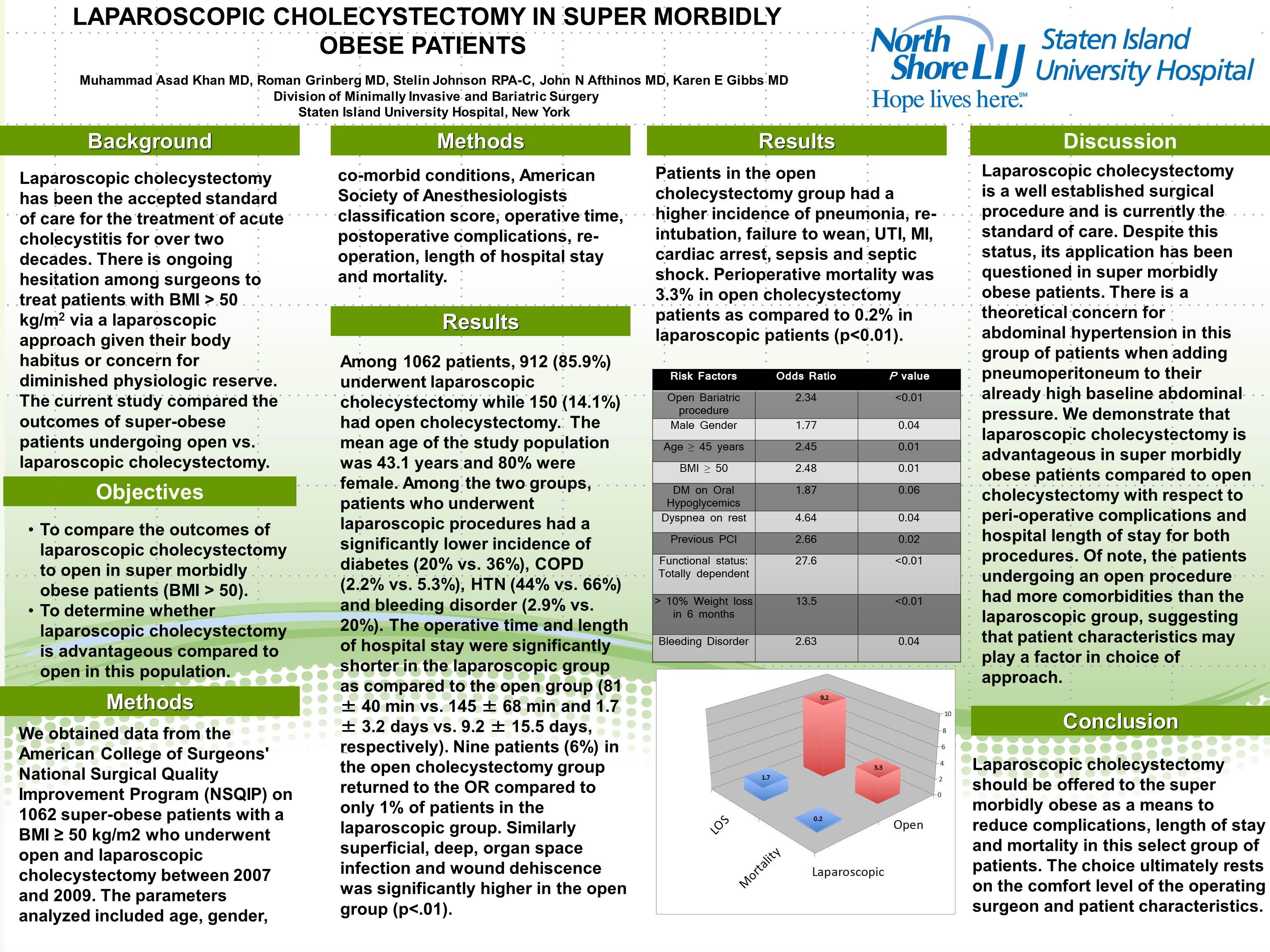
Among 1062 patients, 912 (85.9%) underwent laparoscopic cholecystectomy while 150 (14.1%) had open cholecystectomy. Mean age of the study population was 43.1 years and 80% were female. Among two groups, patients underwent laparoscopic procedures had significantly lower incidence of diabetes (20% vs. 36%), COPD (2.2% vs. 5.3%), HTN (44% vs. 66%) and bleeding disorder (2.9% vs. 20%). Operative time and length of hospital stay was significantly shorter in laparoscopic group as compared to open group (81 ± 40 min vs. 145±68 min and 1.7 ± 3.2 days vs. 9.2 ± 15.5 days, respectively). Nine patients (6%) in open cholecystectomy group underwent return to OR compare to only 1% patients in laparoscopic group. Similarly superficial, deep, organ space infection and wound dehiscence was significantly higher in open group, Patients in open cholecystectomy group had higher incidence of pneumonia, re-intubation, failure to wean, UTI, MI, cardiac arrest, sepsis and septic shock. Perioperative mortality was 3.3% in open cholecystectomy patients as compared to 0.2% in laparoscopic patients (p<0.01).
CONCLUSION:
Laparoscopic cholecystectomy is a safer option for super-obese patients and should be attempted in order to potentially avoid significant peri-operative complications in this high risk group.
| Complications |
Open cholecystectomy N=150 |
Laparoscopic cholecystectomy | P |
|---|---|---|---|
| Reintubation | 8 (5.3%) | 4 (0.4%) | .001 |
| Failure to wean | 11 (7.3%) | 3 (0.3%) | <.001 |
| Progressive renal failure | 7 (4.7%) | 2 (0.2%) | <.001 |
| Urinary tract infection | 4 (2.7%) | 5 (0.5%) | .027 |
| Cardiac arrest | 3 (2%) | 0 (0%) | .003 |
| Myocardial infarction | 2 (1.3%) | 1 (0.1%) | .054 |
| Sepsis | 6 (4%) | 1 (0.1%) | <.001 |
| Septic Shock | 10 (6.7%) | 2 (0.2%) | <.001 |
| Pneumonia | 8 (5.3%) | 4 (0.4%) | <.001 |
Session Number: Poster – Poster Presentations
Program Number: P481
View Poster