James G Bittner IV, MD, Angel M Reyes, MD, Luke G Wolfe, MS, Jill G Meador, RN, BSN, James W Maher, MD, John M Kellum, MD
Department of Surgery, Virginia Commonwealth University Medical Center, Richmond, VA
Introduction: Laparoscopic adjustable gastric banding (LAGB) is considered by many to be a safer and equally effective option compared to laparoscopic Roux-en-Y gastric bypass (LRYGB). Consequently, LAGB quickly became the second most common weight loss operation performed in the United States. Scrutiny of long-term outcomes after LAGB has revealed significant complication and failure rates. We hypothesized that LAGB has higher rates of reoperation, weight loss failure, and overall failure compared to LRYGB at long-term follow-up.
Methods: A matched case-control study was performed using prospectively collected data. Patients who underwent primary LAGB or LRYGB at a university hospital between 2004 and 2011 were matched for age, gender, race, preoperative body mass index (BMI), and the presence of hypertension, diabetes mellitus, obstructive sleep apnea, and hyperlipidemia. All LAGB procedures were performed using the pars flaccida technique. Outcomes included patient demographics, percent excess weight loss (% EWL), BMI units lost, BMI at most recent follow-up, and rates of reoperation, weight loss failure (<50% EWL), and overall failure (procedure-related reoperation and/or <50% EWL) at 3 and 5-year follow-up. Using propensity scoring to select control LRYGB patients, matched cohorts were compared using Chi square and Fisher’s exact tests as appropriate (P<0.05).
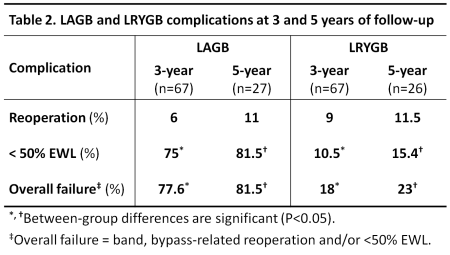
Results: In all, 228 LAGB and 228 LRYGB patients were matched. At 3 and 5 years, LAGB compared to LRYGB patients had a significantly lower % EWL, lost fewer BMI units, and had a higher BMI (Table 1). At longest follow-up, a similar proportion of LAGB and LRYGB patients underwent primary procedure-related reoperation. Rates of weight loss failure were appreciably higher after LAGB than LRYGB at 3 and 5 years (Table 2). This remained true even when weight loss failure was defined as <25% EWL (31.3% vs. 1.5% at 3 years and 81.5% vs. 15.4% at 5 years, both P<0.01). Overall failure rates, defined as procedure-related reoperation and/or <50% EWL, were higher after LAGB at all time points. Band-related complications included erosion (0.4%), port/band infection (0.4%), leak (0.9%), incisional hernia (0.9%), port inversion (0.9%), slippage (7%), and pouch/esophageal enlargement (9.7%). Procedure-related complications after LRYGB were bleeding (1.7%), incisional hernia (2.6%), anastomotic leak (3.5%), and internal hernia (4.8%). Over the study period, morbidity was higher among LAGB compared to LRYGB patients (19 vs. 12.7%, P=0.04). Procedure-related mortality was low after both LAGB (0%) and LRYGB (0.4%).

Conclusions: Based on this single-center study of long-term outcomes, LAGB has similar rates of procedure-related reoperation and significantly higher rates of weight loss failure compared to LRYGB. Additionally, overall failure rates, defined as procedure-related reoperation and/or weight loss failure, are greater after LAGB than LRYGB. While LAGB may be considered for well-informed and motivated patients, these data suggest that long-term effectiveness of LAGB might be limited.
Session: Podium Presentation
Program Number: S117