James A Dickerson, MD, Chan W Park, MD, Dana D Portenier, MD. Duke University Medical Center
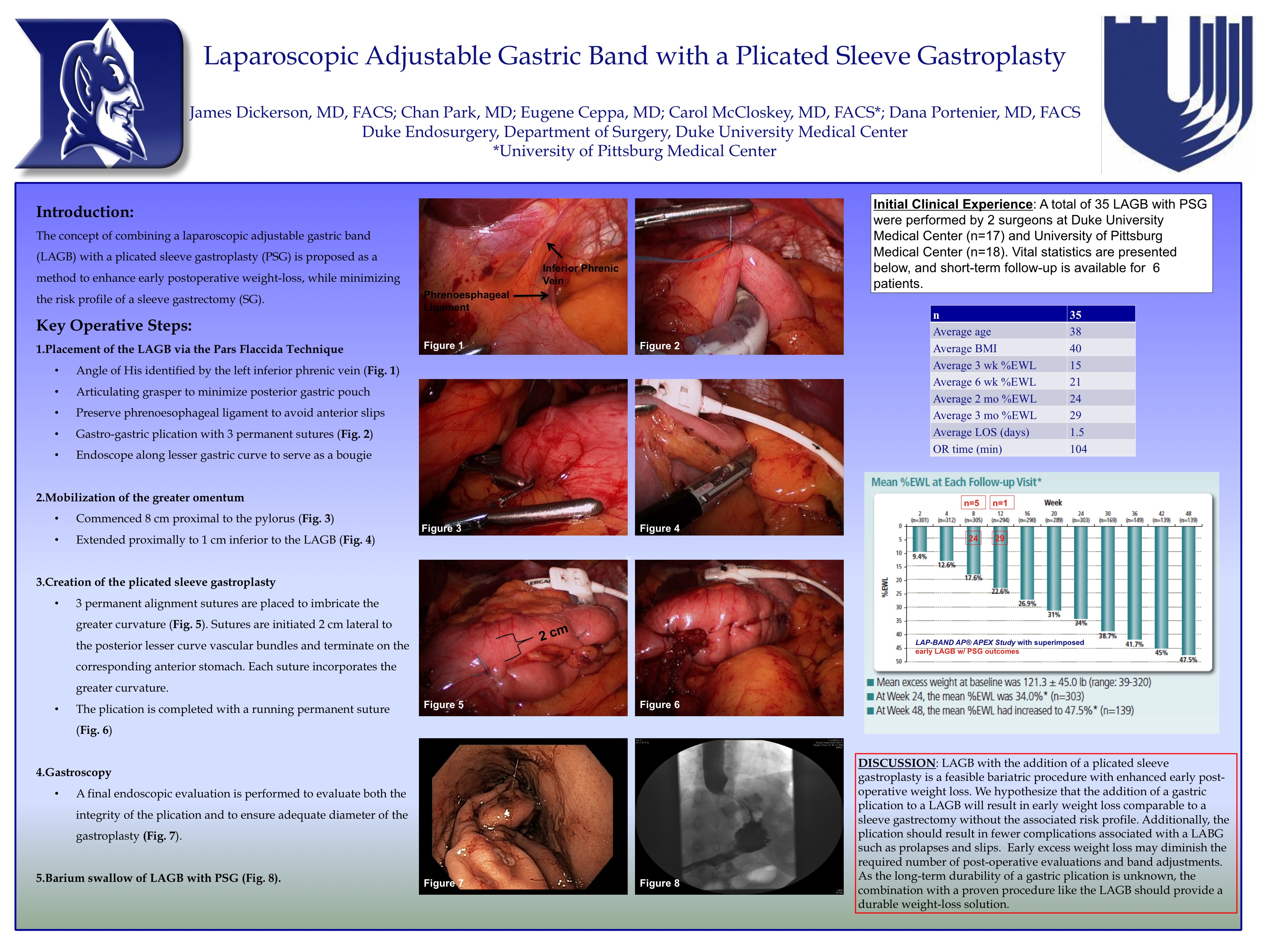
The concept of combining a laparoscopic adjustable gastric band (LAGB) with a plicated sleeve gastroplasty (PSG) is proposed as a method to enhance early postoperative weight-loss, while minimizing the risk profile of a sleeve gastrectomy (SG).
The technique presented depicts a combination of a LAGB with a PSG. The band is placed via the pars flaccida technique. The omentum is mobilized from the greater curve (GC) starting 8 centimeters proximal to the pylorus and ending 2 centimeters distal to the AGB. An endoscope serves as a calibration tube and allows for final evaluation of the gastric sleeve. The GC is invaginated with 3-4 interrupted, non-absorbable alignment sutures. A second running imbrication serves to properly size the gastric tube and ensures the distensible fundus is collapsed.
The operative time for this procedure was 93 minutes with an estimated blood loss of 20 milliliters. There were no intra-operative complications and the patient was discharged on postoperative day one.
There is limited evidence suggesting that short-term weight-loss with a gastric plication is comparable to a sleeve gastrectomy. As the long-term bariatric outcomes of a gastric sleeve have yet to be established, we elected to combine the procedure with an adjustable gastric band. Further longitudinal studies are required to demonstrate the long-term efficacy of a banded sleeve gastroplasty.
Session: Emerging Technology Poster
Program Number: ETP057
View Poster
{kind=link}