Sonia T Orcutt, MD, Christy L Marshall, MD, Courtney J Balentine, MD, Celia N Robinson, MD, Daniel Albo, MD PhD. Department of Surgery, Baylor College of Medicine, Houston, TX
Objective: We present a description of a patient who required an abdominoperineal resection (APR) for resection of rectal cancer involving the anal sphincters. This operation was performed without the use of a perineal incision, as is typically used, to reduce the morbidity of the operation.
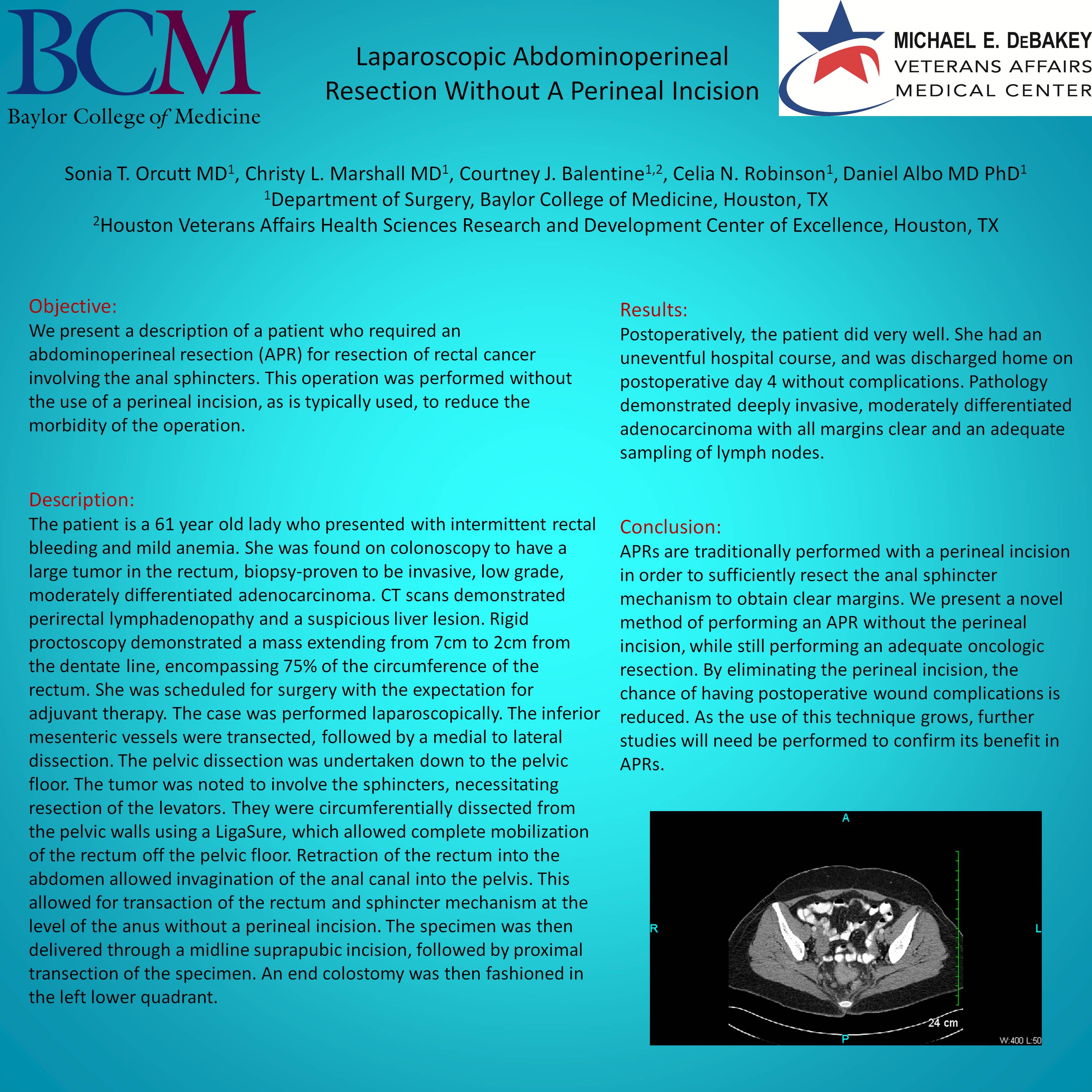
Description: The patient is a 61 year old lady who presented with intermittent rectal bleeding and mild anemia. She was found on colonoscopy to have a large tumor in the rectum, biopsy-proven to be invasive, low grade, moderately differentiated adenocarcinoma. CT scans demonstrated perirectal lymphadenopathy and a suspicious liver lesion. Rigid proctoscopy demonstrated a mass extending from 7cm to 2cm from the dentate line, encompassing 75% of the circumference of the rectum. She was scheduled for surgery with the expectation for adjuvant therapy. The case was performed laparoscopically. The inferior mesenteric vessels were transected, followed by a medial to lateral dissection. The pelvic dissection was undertaken down to the pelvic floor. The tumor was noted to involve the sphincters, necessitating resection of the levators. They were circumferentially dissected from the pelvic walls using a LigaSure, which allowed complete mobilization of the rectum off the pelvic floor. Retraction of the rectum into the abdomen allowed invagination of the anal canal into the pelvis. This allowed for transaction of the rectum and sphincter mechanism at the level of the anus without a perineal incision. The specimen was then delivered through a midline suprapubic incision, followed by proximal transection of the specimen. An end colostomy was then fashioned in the left lower quadrant.
Results: Postoperatively, the patient did very well. She had an uneventful hospital course, and was discharged home on postoperative day 4 without complications. Pathology demonstrated deeply invasive, moderately differentiated adenocarcinoma with all margins clear and an adequate sampling of lymph nodes.
Conclusion: APRs are traditionally performed with a perineal incision in order to sufficiently resect the anal sphincter mechanism to obtain clear margins. We present a novel method of performing an APR without the perineal incision, while still performing an adequate oncologic resection. By eliminating the perineal incision, the chance of having postoperative wound complications is reduced. As the use of this technique grows, further studies will need be performed to confirm its benefit in APRs.
Session: Emerging Technology Poster
Program Number: ETP061
View Poster
{kind=link}