Jason K Sicklick, MD, Michael F Sedrak, MD, Elisabeth C McLemore, MD, Andrew M Lowy, MD, Sonia L Ramamoorthy, MD, Alan W Hemming, MD, Santiago Horgan, MD, Mark A Talamini, MD. Department of Surgery, University of California, San Diego
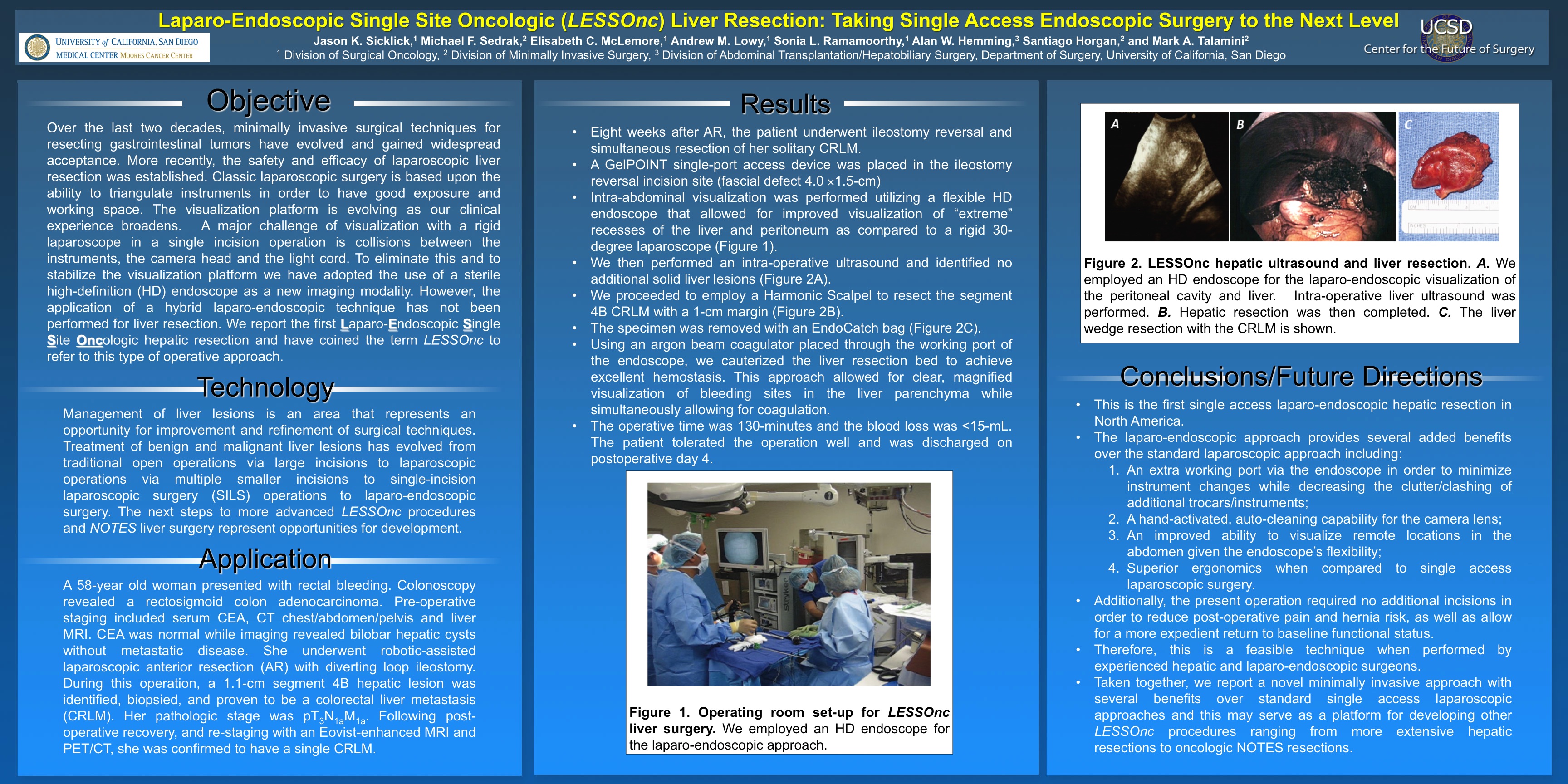
Over the last two decades, minimally invasive surgical techniques for resecting gastrointestinal tumors have evolved and gained widespread acceptance. More recently, the safety and efficacy of laparoscopic liver resection was established. However, the application of a hybrid laparo-endoscopic technique has not been performed for liver resection. We report the first Laparo-Endoscopic Single Site Oncologic hepatic resection and have coined the term LESSOnc to refer to this type of operative approach. TECHNOLOGY/APPLICATION: A 58-year old woman presented with rectal bleeding. Colonoscopy revealed a rectosigmoid colon adenocarcinoma. Pre-operative staging included serum CEA, CT chest/abdomen/pelvis and liver MRI. CEA was normal while imaging revealed bilobar hepatic cysts without metastatic disease. She underwent robotic-assisted laparoscopic anterior resection (AR) with diverting loop ileostomy. During this operation, a 1.1-cm segment 4B hepatic lesion was identified, biopsied, and proven to be a colorectal liver metastasis (CRLM). Her pathologic stage was pT3N1aM1a. Following post-operative recovery, and re-staging with an Eovist-enhanced MRI and PET/CT, she was confirmed to have a single CRLM. RESULTS: Eight weeks after AR, the patient underwent ileostomy reversal and simultaneous resection of her solitary CRLM. A GelPOINT single-port access device was placed in the ileostomy reversal incision site (fascial defect 4.0×1.5-cm). Intra-abdominal visualization was performed utilizing a flexible endoscope that allowed for improved visualization of “extreme” recesses of the liver and peritoneum as compared to a rigid 30-degree laparoscope. We then performed an intra-operative ultrasound and identified no additional solid liver lesions. We proceeded to employ a Harmonic Scalpel to resect the segment 4B CRLM with a 1-cm margin. The specimen was removed with an EndoCatch bag. Using an argon beam coagulator placed through the working port of the endoscope, we cauterized the liver resection bed to achieve excellent hemostasis. This approach allowed for clear, magnified visualization of bleeding sites in the liver parenchyma while simultaneously allowing for coagulation. The operative time was 130-minutes and the blood loss was <15-mL. The patient tolerated the operation well and was discharged on postoperative day 4. CONCLUSIONS/FUTURE DIRECTIONS: This is the first single access laparo-endoscopic hepatic resection. The laparo-endoscopic approach provides several added benefits over the standard laparoscopic approach including: 1) an extra working port via the endoscope in order to minimize instrument changes while decreasing the clutter/clashing of additional trocars/instruments; 2) a hand-activated, auto-cleaning capability for the camera lens; 3) an improved ability to visualize remote locations in the abdomen given the endoscope’s flexibility; and 4) superior ergonomics when compared to single access laparoscopic surgery. Additionally, the present operation required no additional incisions in order to reduce post-operative pain and hernia risk, as well as allow for a more expedient return to baseline functional status. Therefore, this is a feasible technique when performed by experienced hepatic and laparo-endoscopic surgeons. Taken together, we report a novel minimally invasive approach with several benefits over standard single access laparoscopic approaches and this may serve as a platform for developing other LESSOnc procedures ranging from more extensive hepatic resections to oncologic NOTES resections.
Session: Emerging Technology Poster
Program Number: ETP028
View Poster
{kind=link}