B S Brar, MD FRCSC, C Smith, MD FRCSC, I Raiche, MD FRCSC, Jd Yelle, MD FRCSC, J Mamazza, MD FRCSC. University of Ottawa
Introduction: Worldwide obesity rates have been increasing exponentially and bariatric surgery rates have similarly increased to combat this growing epidemic. Previous studies have shown that bariatric surgery can be preformed in a safe manner with low patient morbidity and mortality. What is unclear is the safety and feasibility of early discharge of patients undergoing laparoscopic Roux en Y Gastric Bypass (RYGB). The objective of this study was to examine the impact of early hospital discharge on short-term outcomes of bariatric patients undergoing laparoscopic RYGB.
Methods and Procedure: Retrospective review of patients from November 2007 to July 2011 who had undergone laparoscopic RYGB at the Ottawa Hospital and discharged within the first 3 post operative days. Patients were excluded if there wasn’t sufficient peri-operative data. Discharge readiness was determined by adequate analgesia achieved with PO medication, patients tolerating fluids, voiding well and ambulating without assistance. Fischer exact tests was used to determine if there were any differences between patients discharged on post operative day 1 and those discharged on post operative days 2 or 3.
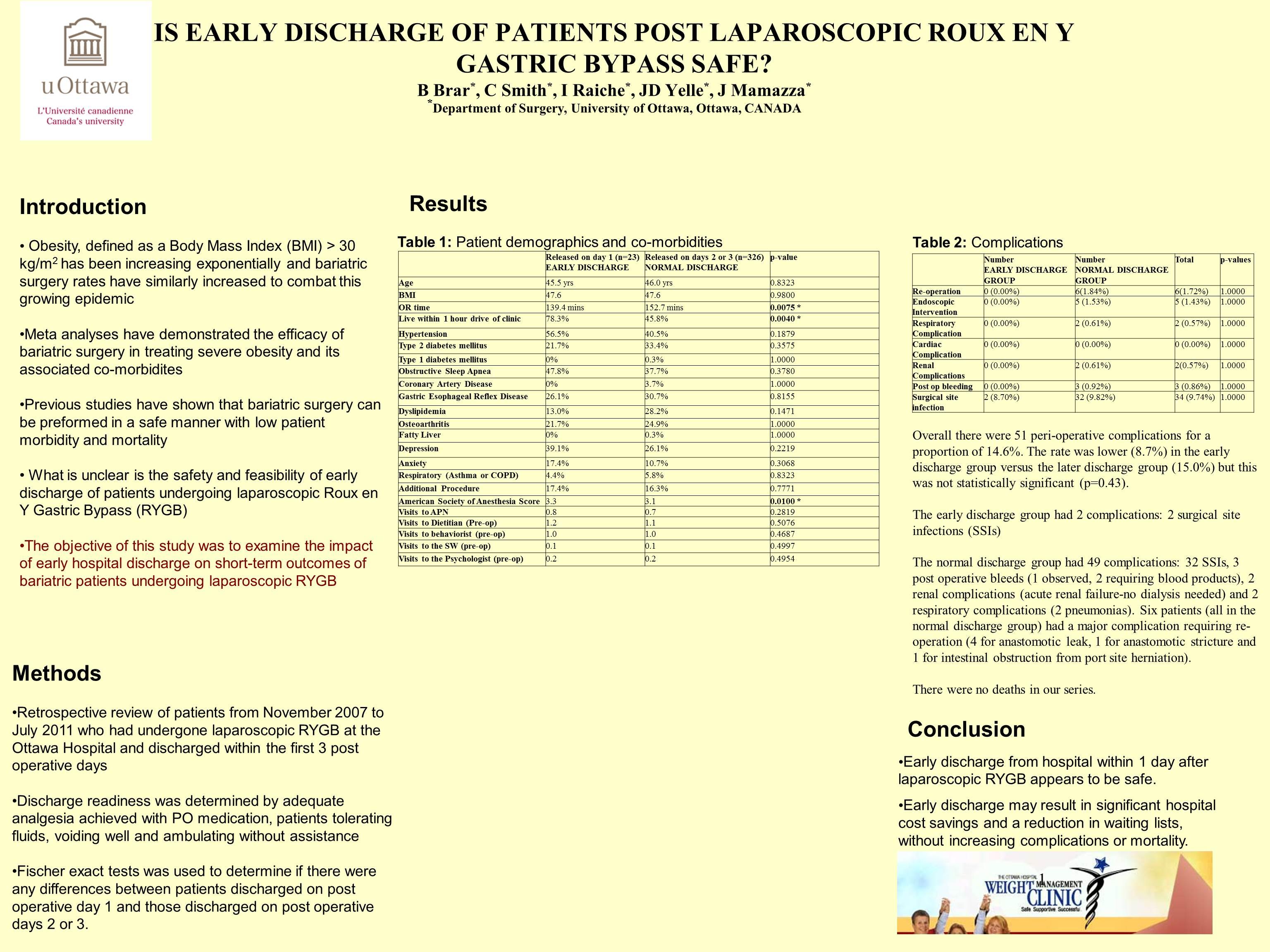
Results: 349 patients (280 females and 69 males) in total were included. 23 were discharged on post operative day 1 (early discharge) with 283 discharged on day 2 and 43 discharged on post operative day 3 (normal discharge). The two groups were similar in terms of mean age (45.5 versus 46.0, p=0.83), mean BMI (47.6 versus 47.6, p=0.98), presence of co morbidities (hypertension, type 1 and 2 diabetes mellitus, obstructive sleep apnea, coronary artery disease, dyslipidemia, gastroesophageal reflux, asthma or COPD). The early discharge group did differ from the normal discharge group in terms of shorter mean operative (139.4 versus 152.7 minutes, p=0.01) and having a significantly greater proportion of patients living within the greater Ottawa area (within 1 hour of travel time to the weight management clinic) (76.3% vs. 45.8%, p=0.004). Overall there were 51 peri-operative complications for a proportion of 14.6%. The rate was lower (8.7%) in the early discharge group versus the later discharge group (15.0%) but this was not statistically significant (p=0.43). The early discharge group only had 2 complications, 2 surgical site infections. The normal discharge group had 49 complications: 32 surgical site infections, 3 post operative bleeds (1 observed, 2 requiring blood products), 2 renal complications (acute renal failure-no dialysis needed) and 2 respiratory complications (2 pneumonias). Six patients (all in the normal discharge group) had a major complication requiring re-operation (4 for anastomotic leak, 1 for anastomotic stricture and 1 for intestinal obstruction from port site herniation). There were no deaths in our series.
Conclusion: Early discharge from hospital within 1 day after laparoscopic RYGB appears to be safe. Early discharge may result in significant hospital cost savings and a reduction in waiting lists, without increasing complications or mortality.
Session Number: Poster – Poster Presentations
Program Number: P478
View Poster