Maitham A Moslim, MD, Gautam Sharma, MD, Hideo Takahashi, MD, Andrew Strong, MD, Mena Boules, MD, Villamere James, MD, O’Rourke Colin, Steven Rosenblatt, MD, Rodriguez John, MD, Kroh Matthew, MD. Cleveland Clinic Foundation
Introduction: Laparoscopic-assisted revision of ventriculoperitoneal (VP) and lumboperitoneal (LP) shunts is an ubiquitous procedure for post-shunt abdominal pain. Complications related to the abdominal portion of the procedure can be managed laparoscopically. The aim of this study is to report a single center experience with laparoscopic distal revision of VP and LP shunts, assessing the resolution of catheter related abdominal symptoms.
Methods: With IRB approval, all patients who underwent distal revision of VP and LP shunts between 1994-2014 were evaluated. The indications for revision, post-operative course, complications and follow-up were documented. Analyses were done using R version 3.2.1.
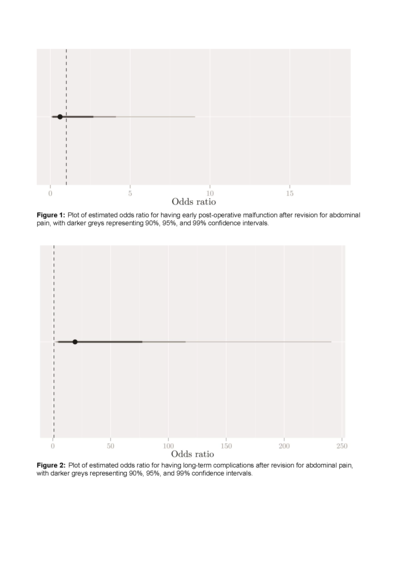
Results: 259 patients underwent distal revision. The indications for revision were: malfunction 49%, infection 21.6%, abdominal pain 16.5%, and others 12.9%. Patients who presented with abdominal pain (n=53) were studies. All revisions were performed on the distal (peritoneal) portion of the catheter; VP to VP, LP to LP and LP to VP (77%, 17% and 6%, respectively). The surgical approach was open, laparoscopic and laparoscopic converted to open (8%, 90% and 6%, respectively). Resolution of abdominal pain was documented in 71.7% of cases, including subsequent revisions (Table 1).
Early post-operative complications included (<30 days): Pain 63%, malfunction 23%, and surgical site infection 14% (n=3). Late complication rates were: pain 35%, malfunction 30% and infection 27% (Table 2). Early post-operative pain was more common in patients who presented with pain for revision (35% vs 18%, P=0.013) (Table 3).
Subsequent revision was performed in 22 patients with total of 53 revisions; median 2 [IQR=3-1]. Common indications were infection (n=21), malfunction (n=17) and abdominal pain (n=8).
With the initial presentation of abdominal pain; the odds of having an early post-operative malfunction, a long-term complication and a larger number of revisions are estimated to be 0.6 (95% CI 0.1-4.1), 19.2 (95% CI 3.2-114.9) and 1.6 (95% CI 0.6-4.1) folds higher for patients without resolution of initial symptoms than for those with resolution; respectively (Fig 1-3).
The median postoperative length of hospitalization was 1 [IQR=1-0] day. The median follow up is 40 [IQR=65-21] months.
Conclusions:The study has demonstrated that patients who present with abdominal pain for distal revision of VP/LP catheter are more inclined to have early postoperative abdominal pain and long-term complications with persistence of pain.