Rodrigo A Pinto, MD, Fábio G Campos, PhD, Sérgio A Araújo, MD, Jaime P Kruger, MD, Guilherme N Namur, MD, Sérgio C Nahas, PhD, Ivan Cecconello. University of São Paulo School of Medicine
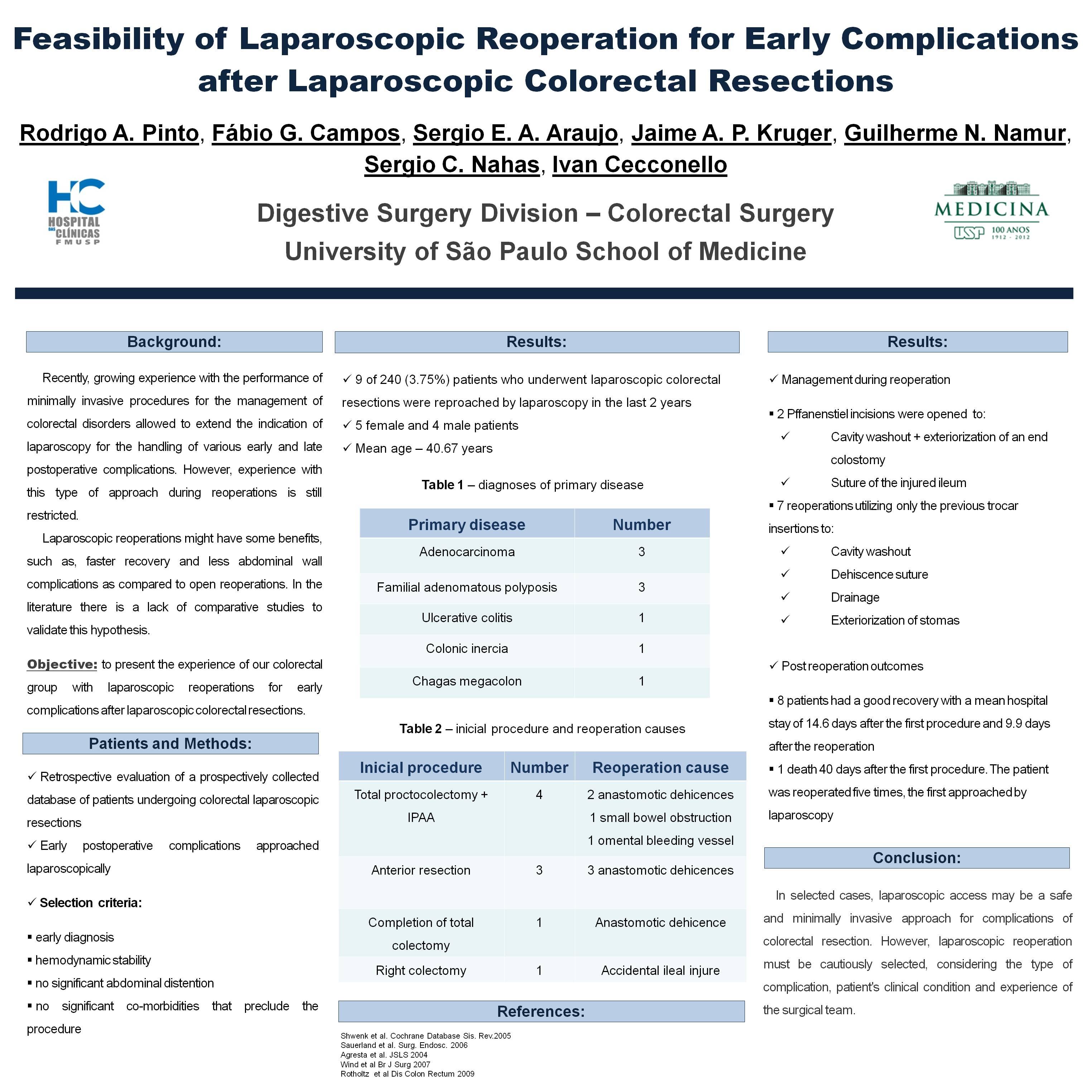
Background: Recently, growing experience with the performance of minimally invasive procedures for the management of colorectal disorders allowed to extend the indication of laparoscopy for the handling of various early and late postoperative complications. However, experience with this type of approach during reoperations is still restricted.
Objective: To present the experience of our colorectal group with laparoscopic reoperations for early complications after laparoscopic colorectal resections.
Methods: A retrospective study of prospectively collected database of patients undergoing laparoscopic colorectal resections that presented postoperative surgical complications that were approached laparoscopically. The patients selected for laparoscopic approch were those with early diagnosis of complications, hemodynamic stability without significant abdominal distention and without clinical comorbidities that would preclude the procedure.
Results: In the last two years, 9 of 240 (3.75%) patients who underwent laparoscopic colorectal resections were reapproached laparoscopically. There were 5 female patients. The mean age was 40.67 years. Diagnoses of primary disease included adenocarcinoma (3), familial adenomatous polyposis (3), ulcerative colitis (1), colonic inertia (1) and Chagássic Megacolon (1). Initial procedures included 4 total proctocolectomy with ileal pouch anal anastomosis, 3 anterior ressections, a completion of total colectomy and a right hemicolectomy. Anastomotic dehiscence was the most common complication that resulted in reoperations (6). An accidental lesion of the ileum, an omental bleeding vessel and a small bowel obstruction were other reasons for reoperation. In two cases, assisting incision had were utilized, one for cleaning the cavity, rectal stump closure and exteriorization of an end colostomy, and another for suture of injured ileum. The other cases were completely laparoscopic, including suture anastomotic dehiscences, and cleaning the cavity with drainage. There was only one case of an unfavorable outcome, with death on the 40th day of the first approach, after consecutive complications and reoperations by 4 other open procedures. The remaining cases had favorable outcome with an average hospital discharge of 14.6 days after the first operation and 9.9 days after reoperation.
Conclusion: In selected cases, laparoscopic access may be a safe and minimally invasive approach for complications of colorectal resection. However, laparoscopic reoperation must be cautiously selected, considering the type of complication, patient’s clinical condition and experience of the surgical team.
Session Number: Poster – Poster Presentations
Program Number: P118
View Poster