Introduction: The purpose of this study is to evaluate the acute and chronic fixation strength of fibrin sealant as an alternative fixation method for laparoscopic ventral hernia repair (LVHR).
Methods: Representative mesh types for LVHR included one nonabsorbable barrier mesh (Composix™), and three absorbable barrier meshes (Sepramesh™, Proceed and Parietex™ Composite). Macroporous polypropylene mesh (Prolite Ultra™) served as control. Three methods of fixation were used, 0-polypropylene suture + fibrin sealant (ARTISS™ 4IU, Baxter Healthcare Corp.), fibrin sealant alone (ARTISS™) or tacks alone, to secure 3x4cm pieces of mesh (n=10 each combination) to the peritoneal surface of New Zealand white rabbit abdominal wall. After 2 hours of incubation at 37C, specimens underwent acute testing, described below. Subsequently, a chronic phase was completed using the aforementioned fixation methods (n=10 each combination), where two 4x4cm pieces of mesh were secured intraperitoneally in each of 75 New Zealand white rabbits and survived eight weeks until sacrifice. A transparent grid overlay was utilized to measure mesh area and adhesion area. Adhesion tenacity was characterized using the Garrard adhesion scale. For both acute and chronic samples, a 3x3cm area of mesh-tissue interface underwent lap shear testing at a rate of 0.42mm/sec using a tensiometer (Instron 5542, Norwood, MA), for both acute and chronic samples. The maximum load sustained by the mesh-tissue construct was recorded as the acute fixation strength in Newtons (N). Data are given as means ± SEM. Statistical significance (p<0.05) was determined using a one-way ANOVA with Fisher’s LSD post-test or a nonparametric Kruskal-Wallis test (adhesion scores).
Results: Acute fixation strength was significantly greater for all meshes secured with either suture + ARTISS™ or tacks alone compared to ARTISS™ alone (p<0.001 for all comparisons). All meshes except Proceed demonstrated greater acute fixation strength with suture + ARTISS™ compared to tacks alone (p<0.05). Composix™ achieved greater acute fixation with suture and ARTISS™ compared to all other meshes (p≤0.029). Acute fixation with suture + ARTISS™ was greater for Parietex™ Composite and ProLite Ultra™ compared to Proceed (p≤0.020). Upon sacrifice, 48 out of 50 meshes fixed with ARTISS™ alone were insufficiently affixed to the abdominal wall, which may have resulted in hernia recurrence in a hernia model. Chronic fixation strength was greater for all mesh types with suture + ARTISS™ compared to ARTISS™ alone (p≤0.023). Chronic fixation strength was greater for tacks compared to ARTISS™ alone for Composix™, Sepramesh™, and Parietex™ Composite (p≤0.012). Chronic fixation strength was greater for suture + ARTISS™ compared to tacks for Proceed and ProLite Ultra™ (p≤0.017). There were no significant differences regarding mesh area, adhesion area or adhesion tenacity, for any mesh/fixation method combination.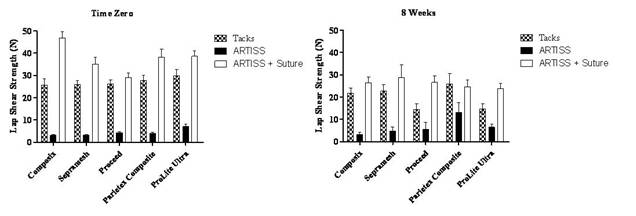
Conclusions: In a chronic rabbit model of LVHR, fixation strength with fibrin sealant alone was inadequate for selected nonabsorbable and absorbable barrier-coated meshes. Acute and chronic fixation strengths of suture + fibrin sealant were equivalent or superior to fixation strength of tacks alone. In this preclinical series, fibrin sealant alone to secure mesh to the peritoneal surface may have led to early recurrence.
Session: Podium Presentation
Program Number: S022