Lorenzo E Ferri, MD PhD, Gerald Fried, MD. McGill University and The Steinberg-Bernstein Centre for Minimally Invasive Surgery
Objective:
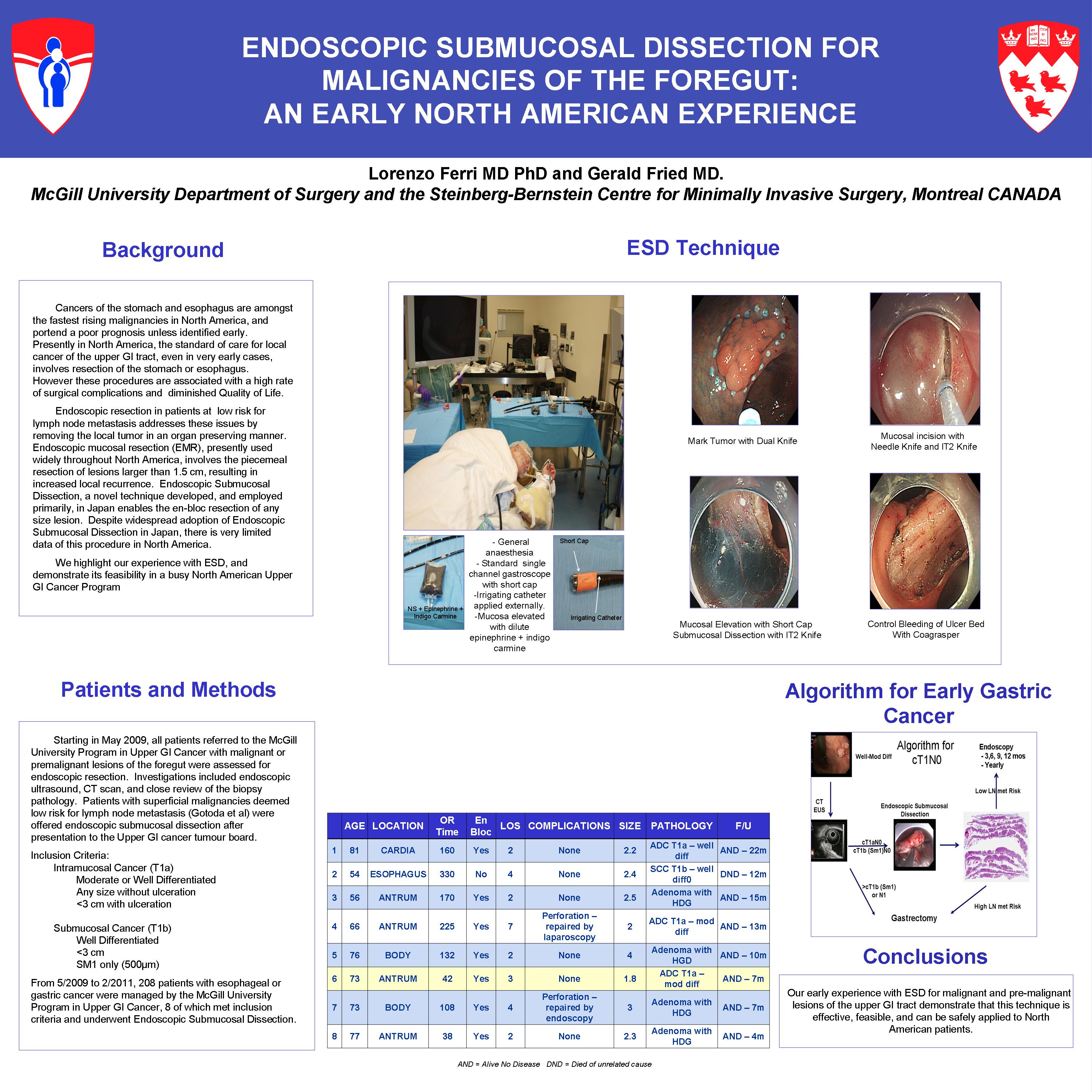
Endoscopic resection of early malignancies of the GI tract is justified in patients with a negligible risk of lymph node metastasis. Endoscopic Submucosal Dissection (ESD) enables the organ-sparing and en-bloc resection of any size lesion, significantly reducing the high rate of local recurrence seen with Endoscopic Mucosal Resection (EMR). ESD is presently used in Japan and Korea, but there is very limited North American data on this technique. We highlight our experience with ESD, and demonstrate its feasibility in a busy North American Upper GI Cancer Program
Description of the Technology:
ESD employs specialized electrocautery needle knives passed through the operating channel of standard therapeutic endoscopes fitted with a short extension cap. After marking the margins with electrocautery, the lesion is elevated from the muscularis propria by submucosal injection of a dilute epinephrine solution. A complete mucosal incision is generated with an insulated tip needle knife, and the submucosa is then dissected directly off of the muscularis propria, removing the specimen in an en-bloc manner.
Preliminary Results:
From 6/2009-10/2010, 7 highly selected pts, 66y (54-81), presenting to an North American academic upper GI cancer program harboring malignant or pre-malignant lesions of the stomach and esophagus with a negligible risk of lymph node metastasis (grade 1, no LVI, no ulceration) underwent ESD after endoscopic ultrasound and CT scan. One proximal esophageal and 6 gastric tumors (cardia =1, body = 2, antrum = 3) were resected under general anesthesia in 151 min. (42-330). Two complications occurred, both minor gastric perforations repaired endoscopically x1(clip) and laparoscopically x1. LOS was 3 days(2-7). 6/7 lesions were resected en-bloc and final pathology revealed completely resected well or mod. diff. carcinoma (ADC=3:SCC=1) in 4 pts (T1a=3:T1b=1), and adenoma with high grade dysplasia in 3 pts. At 9 mos (3-18) follow up, no patient has recurred on serial (Q3mos) follow up.
Conclusions:
Our early experience with ESD for malignant and pre-malignant lesions of the upper GI tract demonstrate that this technique is effective, feasible, and can be safely applied to North American patients.
Session: Emerging Technology Poster
Program Number: ETP094
View Poster
{kind=link}