Abdelrahman A Nimeri, MD, Maria Margarita, MD, Mohammed B Al Hadad, RN. SKMC managed by Cleveland Clinic
Sleeve gastrectomy is considered a primary treatment for morbid obesity. Leaks following sleeve gastrectomy are not uncommon, and may lead to major morbidity, and prolonged hospital stay.2 The leak rate from gastric staple line ranges from 1.4 – 20% Endoscopic stent placement is a potential management strategy. However, it requires expertise, may not heal the leak, lead to stent migration, or significant dysphagia in some patients. A standard method of managing leaks following sleeve gastrectomy has not been established.
Objective:
To evaluate the outcomes of consecutive patients with leaks following laparoscopic sleeve gastrectomy managed at BMI Abu Dhabi.
Methods:
We performed a retrospective analysis of our prospectively maintained data base of consecutive patients with leaks after laparoscopic sleeve gastrectomy managed at BMI Abu Dhabi utilizing a standardized operative management strategy without the use of endoscopic stenting between April 2010 and April 2011. All patients were optimized, and resuscitated adequately before surgery. Data was obtained from the hospital medical record, and IRB approval was obtained.
Results:
All patients were referred to BMI Abu Dhabi; during the same time period we performed 34 laparoscopic sleeve gastrectomies without a leak. We identified a total of four patients. Two patients were done at a private hospital in the UAE, one done in Jordan, and one in Egypt. All patients were referred for higher level of care. All patients were optimized, and resuscitated adequately before surgery. Intraoperatively, all patients had endoscopy and a T tube was placed into the leak if identified clearly; Otherwise, the area of the leak was drained adequately and a jejunostomy tube was inserted in a standard fashion. No attempts were made at suturing the leak site. All leaks healed following an initial period of inpatient hospital stay, followed by an outpatient period on jejunostomy tube feeding and Nil Per Os (NPO). All Leaks healed without the need for endoscopic stent placement.
Conclusion:
Early single stage operative management of leaks after laparoscopic sleeve gastrectomy utilizing a standardized operative strategy without the use of endoscopic stenting is both safe and effective.
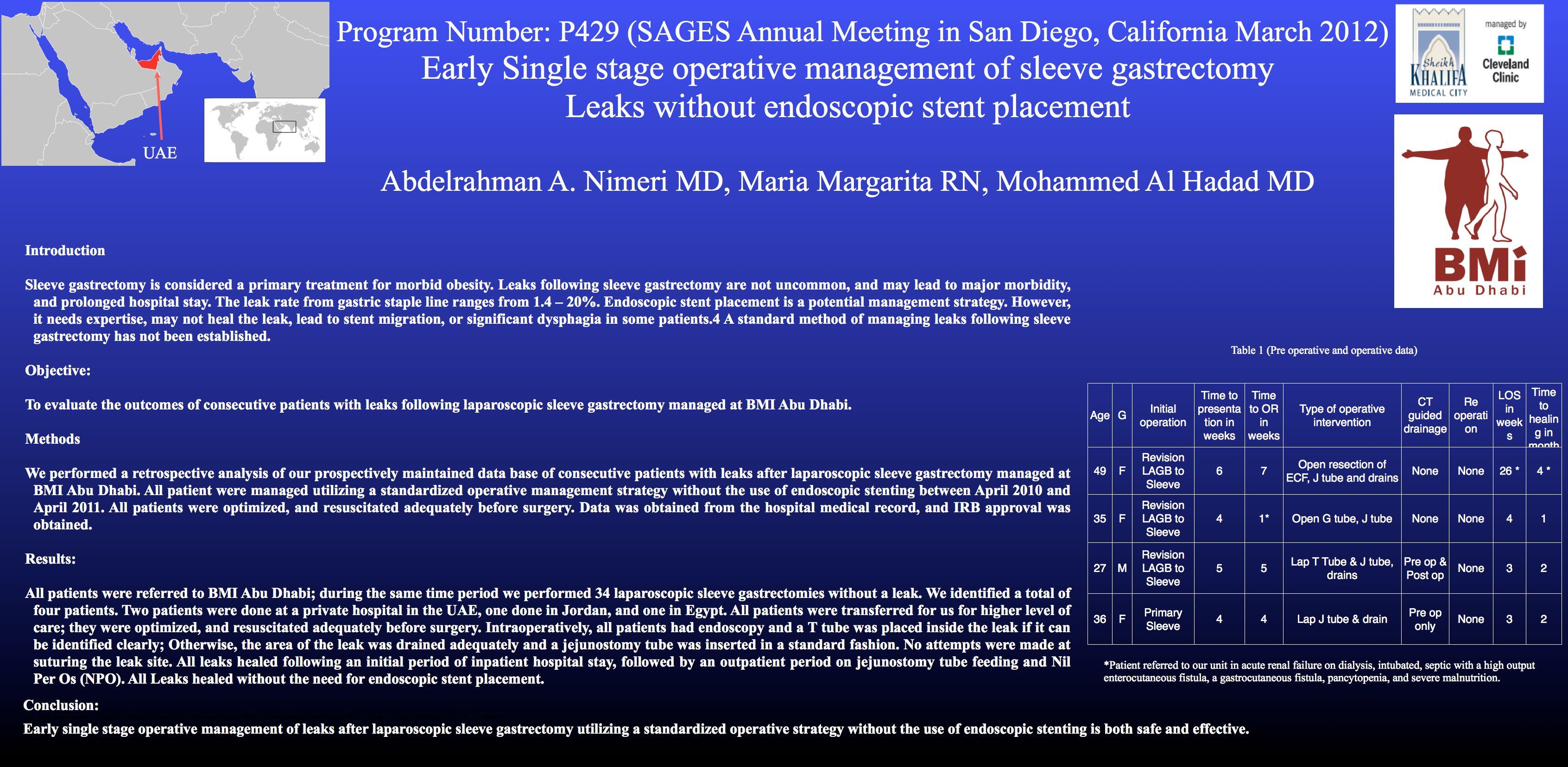
| Age | Sex | Time to presentation to BMI Abu Dhabi | Initial operation | Time to Surgery | Operative strategy |
| 49 | F | 6 weeks | Revision of LAGB to sleeve | 7 weeks | Open SB resection, ECF resection, J tube |
| 35 | M | 4 weeks | Revision of LAGB to sleeve | 1 weeks | Open G tube, J tube |
| 27 | F | 5 weeks | Revision of LAGB to sleeve | 5 weeks | Lap T Tube & J tube, drains |
| 36 | F | 4 weeks | Primary Sleeve | 4 weeks | Lap J tube & drain |
| Radiological drainage | Reoperation | LOS | Time to leak closure | Outcome |
| None | None | 26 weeks | 16 weeks | Healed |
| None | None | 4 weeks | 4 weeks | Healed |
| Pre and post surgery | None | 4 weeks | 8 weeks | Healed |
| Pre surgery only | None | 4 weeks | 8 weeks | Healed |
*Patient referred to our unit in acute renal failure on dialysis, intubated, septic with a high output enterocutaneous fistula, a gastrocutaneous fistula, pancytopenia, and severe malnutrition.
Session Number: Poster – Poster Presentations
Program Number: P429
View Poster