U Khater, G da Silva, S D Wexner, D Sands, J J Nogueras, D Maron, L Rosen, E G Weiss. Cleveland Clinic Florida
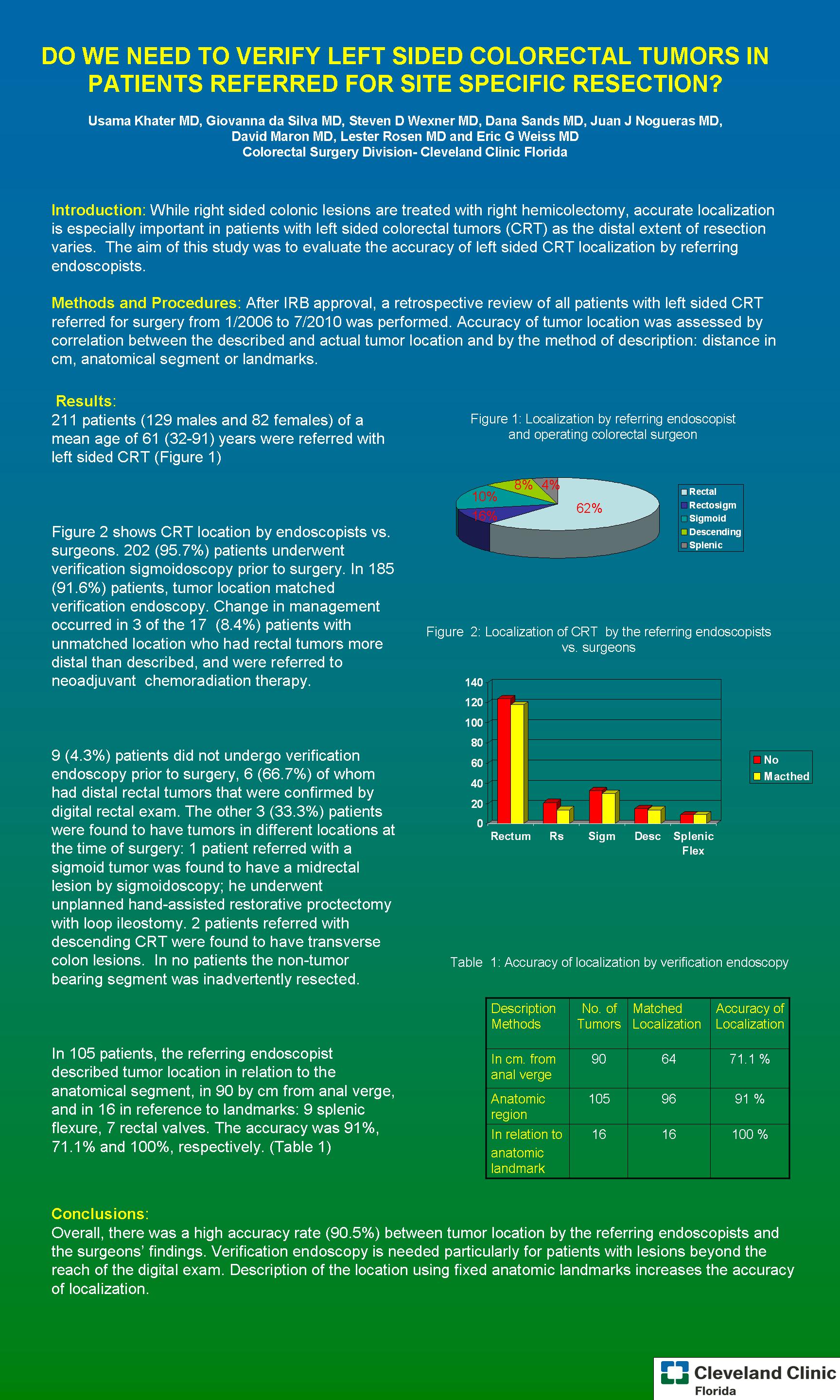
Introduction: While right sided colonic lesions are treated with right hemicolectomy, accurate localization is especially important in patients with left sided colorectal tumors (CRT) as the distal extent of resection varies. The aim of this study was to evaluate the accuracy of left sided CRT localization by referring endoscopists by correlation between the described and actual tumor location, and by the method of description: distance in cm, anatomical segment or landmarks.
Methods and Procedures: After Institutional Review Board approval, a retrospective review of all patients with left sided CRT referred for surgery from 1/06 to 7/10 was performed. Tumor location was compared with endoscopic findings by the surgeon in the office. The description method in the endoscopic report was correlated with the actual tumor location.
Results: 211 patients (129 males and 82 females) of a mean age of 61 (32-91) years were referred with left sided CRT. 202 (95.7%) patients underwent verification sigmoidoscopy prior to surgery. In185 (91.6%) patients, tumor location matched verification endoscopy. 3 of the 17 (8.4%) patients with unmatched location had a change in management, all of whom had rectal tumors more distal than described by the endoscopist, and were referred to neoadjuvant chemoradiation therapy. Nine (4.3%) patients did not undergo verification sigmoidoscopy prior to surgery, 6 (66.7%) of whom had distal rectal tumors that were confirmed by digital rectal exam. The other 3 (33.3%) patients had tumors more proximal than described in the endoscopic report. One patient, referred with a sigmoid tumor required intraoperative colonoscopy, which revealed a midrectal lesion; he underwent a hand-assisted restorative proctectomy with loop ileostomy. Two patients referred with descending CRT were found to have transverse colon lesions. One of them required intraoperative colonoscopy as the tumor could no be palpated after laparotomy. The other patient underwent laparoscopic left hemicolectomy after identification of the tattoo in the splenic flexure, without the need of colonoscopy. In no patients the non-tumor bearing segment was inadvertently resected. In 105 patients, the referring endoscopist described tumor location in relation to the anatomical segment, in 90 by cm from anal verge, and in 16 in reference to landmarks: 9 splenic flexure, 7 rectal valves. The accuracy was 92.1%, 71.1% and 100%, respectively.
Conclusions: Overall, there was a high accuracy rate (90.5%) between tumor location by the referring endoscopists and the surgeons’ findings. Verification endoscopy is needed particularly for patients with lesions beyond the reach of the digital exam. Description of the location using fixed anatomic landmarks increases the accuracy of localization
Session: Poster
Program Number: P154
View Poster
{kind=link}