Christina L Greene, MD, Steven R DeMeester, MD, Joerg Zehetner, MD, Daniel S Oh, MD, Jeffrey A Hagen, MD
Keck Hospital of the University of Southern California, Los Angeles, CA
INTRODUCTION: Laparoscopic paraesophageal hernia (PEH) repair is associated with a high recurrence rate. In a recent randomized trial the recurrence rate exceeded 50% at five years. Similar to repair of other hernias, minimizing tension is a critical factor in preventing recurrence with PEH repair. At the hiatus, tension can occur secondary to a shortened esophagus or widely splayed crura. A Collis-Gastroplasty can address esophageal shortening while diaphragmatic relaxing incisions can address crural tension. The aim of this study is to describe the technique and review the outcomes of laparoscopic diaphragmatic relaxing incisions in patients undergoing PEH repair.
METHODS AND PROCEDURES: Records were reviewed to identify patients who had a relaxing incision during laparoscopic PEH repair. We considered patients to have a PEH when 50% or more of the stomach was intra-thoracic. The right relaxing incision was performed by opening the right crus next to the inferior vena cava, saving a 3 mm cuff of tissue along the cava to allow a patch to be sewn into place. The incision was full-thickness into the right pleural space, starting halfway up the right crus and stopping just below the anterior crural vein (Figure 1). The left relaxing incision starts lateral to the hiatus and follows the course of the rib laterally, typically beyond the spleen (Figure 2). The defect in each case was repaired with a suitably sized 1 mm Gortex patch (Figure 3 & 4). Patients were followed by chest X-Ray and videoesophagram at three months and annually.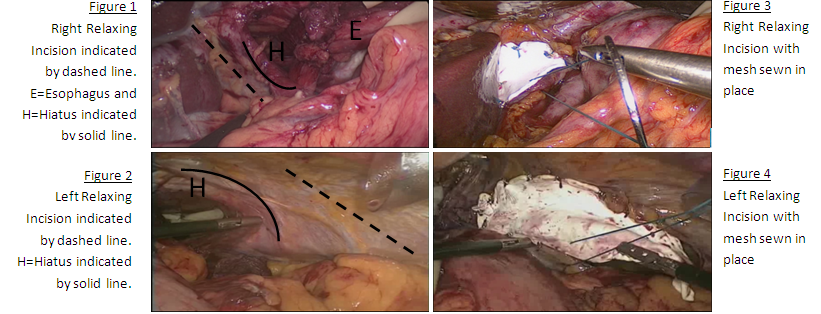
RESULTS: From November 2010 to May 2012, 57 patients had PEH repair and 12 had a relaxing incision to accomplish crural closure. Eight patients were women and four were men, with a mean age of 72 years (58-84). The relaxing incision was right-sided in ten, left-sided in one and bilateral in one patient. All procedures were completed laparoscopically and included a fundoplication. In six patients a wedge- fundectomy Collis-Gastroplasty was performed. There were no major complications. At a median follow-up of 11.8 months, one patient had an asymptomatic mildly elevated right hemidiaphragm. All 12 patients had intact fundoplications without recurrent hiatal hernia or evidence of diaphragmatic disruption.
CONCLUSION: Crural tension likely contributes to the high recurrence rate noted with laparoscopic PEH repair. Relaxing incisions allow crural approximation with good short term outcomes and no major complications. Advanced laparoscopic surgeons should be aware of this option when faced with a large hiatus in a patient with PEH.
Session: Podium Presentation
Program Number: S063