Objective of Study
Avascular anatomical planes guided surgery is an important prerequisite for expeditious & safe procedure. These so called “holy planes” are of help in performing Laparoscopic cholecystectomy (LC). We have earlier reported technique of LC without any energised dissection (ED) and its replication by a higher surgical trainee (HST). The HST had an earlier experience of performing LC with the help of ED. We studied the feasibility of LC without ED, performed by a basic surgical trainee (BST) having not done any independent LC before.
Methods and procedures
From July 2006 to June 2008, Fifty unselected consecutive volunteer candidates for day care LC on index hospital presentation were prospectively randomized to be operated by either a consultant (control group) or a BST (study group). First 3 years of 6 year surgical training are known as basic surgical training.
The patients were operated without ED on day care surgery basis following a standard ethics and informed consent protocol after standard hemato-biochemical and pre-anesthesia evaluation. The operating surgeons were blind to per / peri and post-operative evaluation which was done by an independent anesthetist. Feasibility & the safety of BST performed LC was studied by Per-operative* and Post-operative# Endpoints as shown in Table 1 & 2 respectively.
Results
The Study & Control groups were well matched with respect to demographic, co-morbidity and gallbladder inflammation parameters. BST could complete all procedures safely without any technical difficulty under the Camera holding Consultant’s supervision. The duration of surgery was comparatively longer in the Study group as the BST was inexperienced in LC before the start of this study.
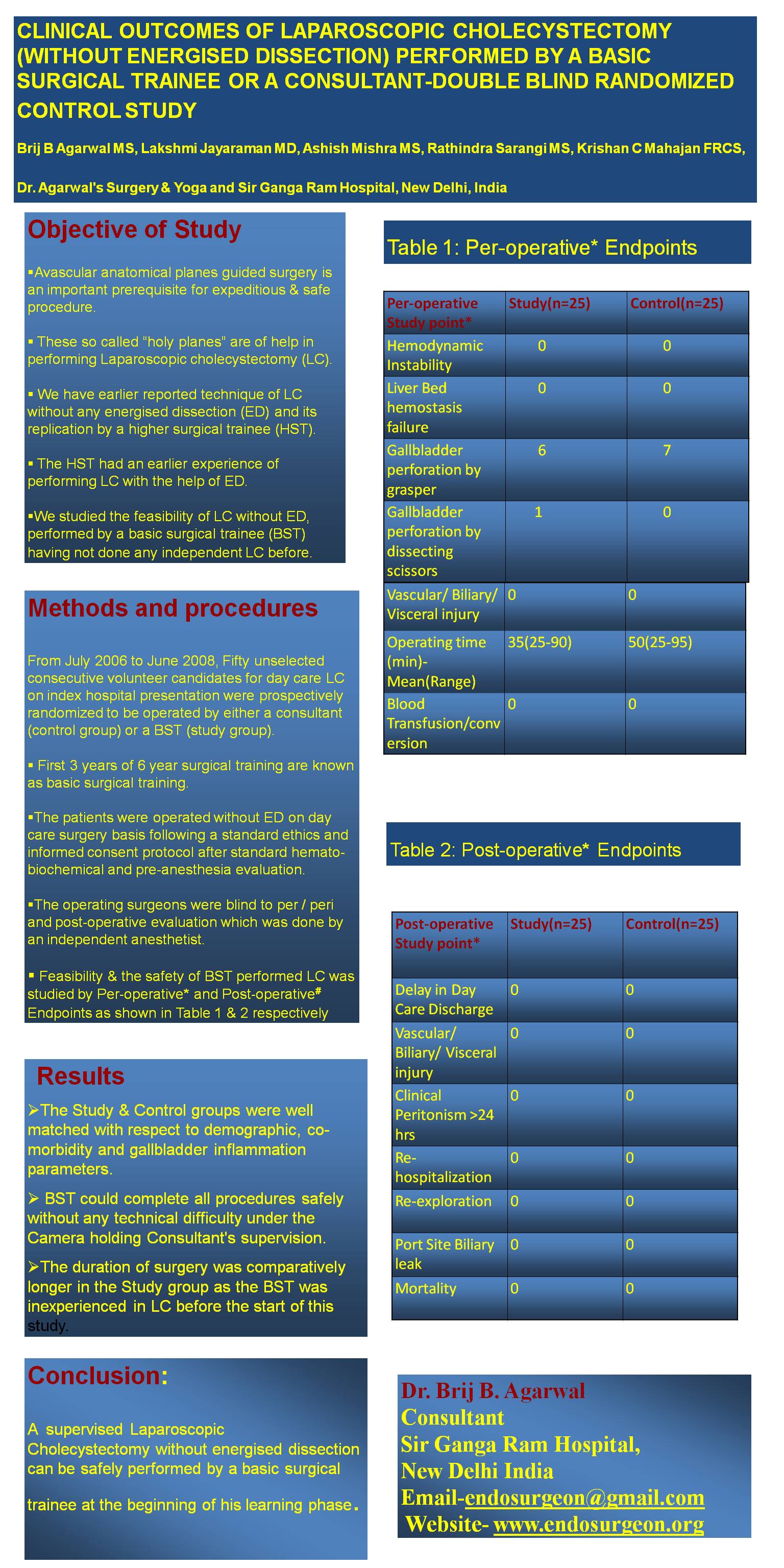
Table 1: Per-operative* Endpoints
| Per-operative Study point* | Study(n=25) | Control(n=25) |
| Hemodynamic Instability | 0 | 0 |
| Liver Bed hemostasis failure | 0 | 0 |
| Gallbladder perforation by grasper | 6 | 7 |
| Gallbladder perforation by dissecting scissors | 1 | 0 |
| Vascular/ Biliary/ Visceral injury | 0 | 0 |
| Operating time (min)- Mean(Range) | 35(25-90) | 50(25-95) |
| Blood Transfusion/conversion | 0 | 0 |
Table 2: Post-operative# Endpoints
| Post-operative Study Point# | Study (n=25) | Control(n=25) |
| Delay in Day Care Discharge | 0 | 0 |
| Vascular/ Biliary/ Visceral injury | 0 | 0 |
| Clinical Peritonism >24 hrs | 0 | 0 |
| Re-hospitalization | 0 | 0 |
| Re-exploration | 0 | 0 |
| Port Site Biliary leak | 0 | 0 |
| Mortality | 0 | 0 |
Conclusion:
A supervised Laparoscopic Cholecystectomy without energised dissection can be safely performed by a basic surgical trainee at the beginning of his learning phase.
Session: Poster
Program Number: P407