David Bunting, Mr, Lukasz Szczebiot, Dr, Paul Peyser, Mr. The Royal Cornwall Hospital, Truro, Cornwall, UK.
Introduction
The benefits of anti-reflux surgery are well established. Laparoscopic techniques have been shown to be generally safe and effective. Whilst some postoperative discomfort is common, a small percentage of patients suffer persistent and severe pain after anti-reflux surgery. There is limited discussion of this in the literature, no established scheme for managing these patients and little is known about the cause of the pain. This study reviews the literature on pain following laparoscopic anti-reflux surgery. An algorithm for its investigation and treatment is constructed. The authors present two cases previously undescribed of postoperative pain following laparoscopic fundoplication caused by traumatic neuromas.
Methods and procedures
A systematic review of the literature without date restriction using the PubMed database was conducted to identify all studies reporting pain after anti-reflux surgery. Other important studies were identified by cross-checking reference lists and using the related articles feature. Studies were included for the main analysis if they contained at least 30 patients operated on for gastro-esophageal reflux disease. Operations in children, Collis gastroplasty procedures, endoluminal fundoplication and surgery for paraoesophageal hernias were excluded. The frequency, severity, cause, duration, investigation and treatment of post-operative pain are discussed. An algorithm for the investigation and management of patients with pain following laparoscopic fundoplication is presented.
Results
256 individual studies were identified through the initial search. After the application of specified criteria, 18 studies were included in the main analysis containing a total of 2769 patients. The frequency of abdominal pain following fundoplication ranged from 1% to 58% (mean 24.0%). Chest pain occurred in 2.4% to 41% (mean 19.5%) of patients. Frequency of pain did not correlate with follow up length (p=0.24) and was not associated with operation type. Meta-analysis was not possible due to the heterogeneity of studies and the small number of comparative studies. Pain was mild or moderate in the majority and severe in 4% of patients who underwent surgery. In the group of patients with severe pain, there was often limited further investigation and no diagnosis made.
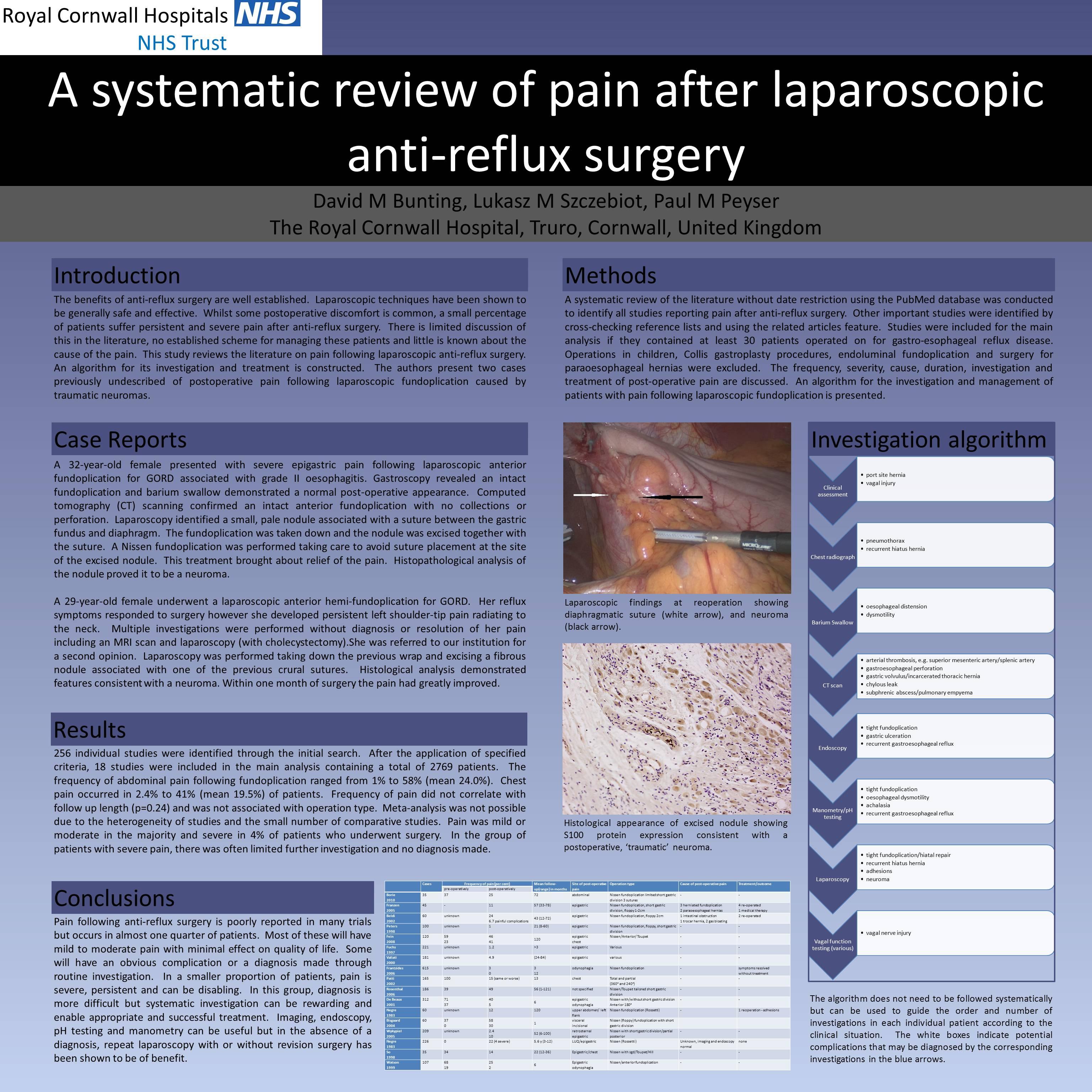
The authors present two cases of persistent, severe epigastric pain following laparoscopic anterior fundoplication. Initial investigations failed to identify any cause. Laparoscopy in each case demonstrated a small, pale nodule associated with a gastric fundal suture. Pain was alleviated by excising the nodules. Histopathological analysis of both lesions proved them to be neuromas.
Conclusions
Pain following anti-reflux surgery is poorly reported in many trials but occurs in almost one quarter of patients. Most of these will have mild to moderate pain with minimal effect on quality of life. Some will have an obvious complication or a diagnosis made through routine investigation. In a smaller proportion of patients, pain is severe, persistent and can be disabling. In this group, diagnosis is more difficult but systematic investigation can be rewarding and enable appropriate and successful treatment. Imaging, endoscopy, pH testing and manometry can be useful but in the absence of a diagnosis, repeat laparoscopy with or without revision surgery has been shown to be of benefit.
Session Number: Poster – Poster Presentations
Program Number: P226
View Poster