Joo-ho Lee, MD PhD, Joo Hyun Woo, MD. Ewha Womans University School of Medicine
INTRODUCTION Most surgeons have performed laparoscopy-assisted distal gastrectomy (LADG) with extracorporeal anastomosis rather than total laparoscopic procedures because of the technical difficulties of intracorporeal anastomosis. However, recently totally laparoscopic distal gastrectomy (TLDG) has been reported to be safe, technically feasible, and more minimally invasive. We conducted this study to compare the short-term outcomes of LADG with TLDG to provide the basis for standardization of laparoscopic gastrectomy in early gastric cancer.
METHODS AND PROCEDURES In this prospective study, 35 patients with early gastric cancer were randomized to either TLDG or LADG with Billroth II anastomosis from February to August 2001. Clinicopathologic characteristics, operative details, postoperative course and quality of life were compared between two groups. Postoperative pain intensity at rest was measured on 100-mm visual analogue scale during hospital stay. Test of pulmonary function was performed on preoperative day and postoperative day 4. Quality of life was assessed using EORTC QLQ-C30, version 3 and the gastric module STO22 on first visit for follow-up after discharge. Approval of the institutional review board and written informed consent were obtained.
RESULTS
| TLDG (n=18) | LADG (n=17) | P-value | |
| Operative details | |||
| Operative time (min) | 131.3±90.3 | 233.1±42.0 | 0.08 |
| Estimated blood loss (mL) | 131.3±90.3 | 153.8±82.8 | 0.50 |
| Stapler devices used | 4.2±1.1 | 2.0±0.0 | 0.01 |
|
The longest length of woundafter skin closure (cm) |
3.3±1.4 | 5.2±1.1 | 0.02 |
| Postoperative course | |||
| Postoperative pain score on day 5 |
2.5±7.1 | 2.0±4.2 | 0.85 |
| Opioid consumption added to intravenous PCA |
1.9±2.5 | 2.6±1.8 | 0.51 |
| First flatus (days) | 3.1±1.0 | 2.8±0.9 | 0.56 |
| Liquid diet (days) | 4.2±1.1 | 3.8±0.7 | 0.34 |
| Postoperative hospital stay (days) | 8.1±3.1 | 7.4±1.7 | 0.49 |
| Pulmonary function | |||
| Decreased forced vital capacity (%) | 19.8±12.3 | 20.8±17.0 | 0.87 |
| Decreased forced expiratory volume in 1 second (%) |
15.4±10.6 | 16.7±12.0 | 0.75 |
| Quality of life |
|||
| Physical function | 81.7±6.4 | 67.5±13.5 | 0.03 |
| Global health | 66.7±13.6 | 61.5±14.7 | 0.57 |
| Pain and discomfort | 22.2±20.3 | 29.2±10.2 | 0.56 |
| Emotional problem | 22.2±15.7 | 27.8±16.8 | 0.59 |
| Restriction of eating | 27.1±18.5 | 27.8±16.8 | 0.84 |
| Body image | 24.9±31.9 | 29.2±27.8 | 0.82 |
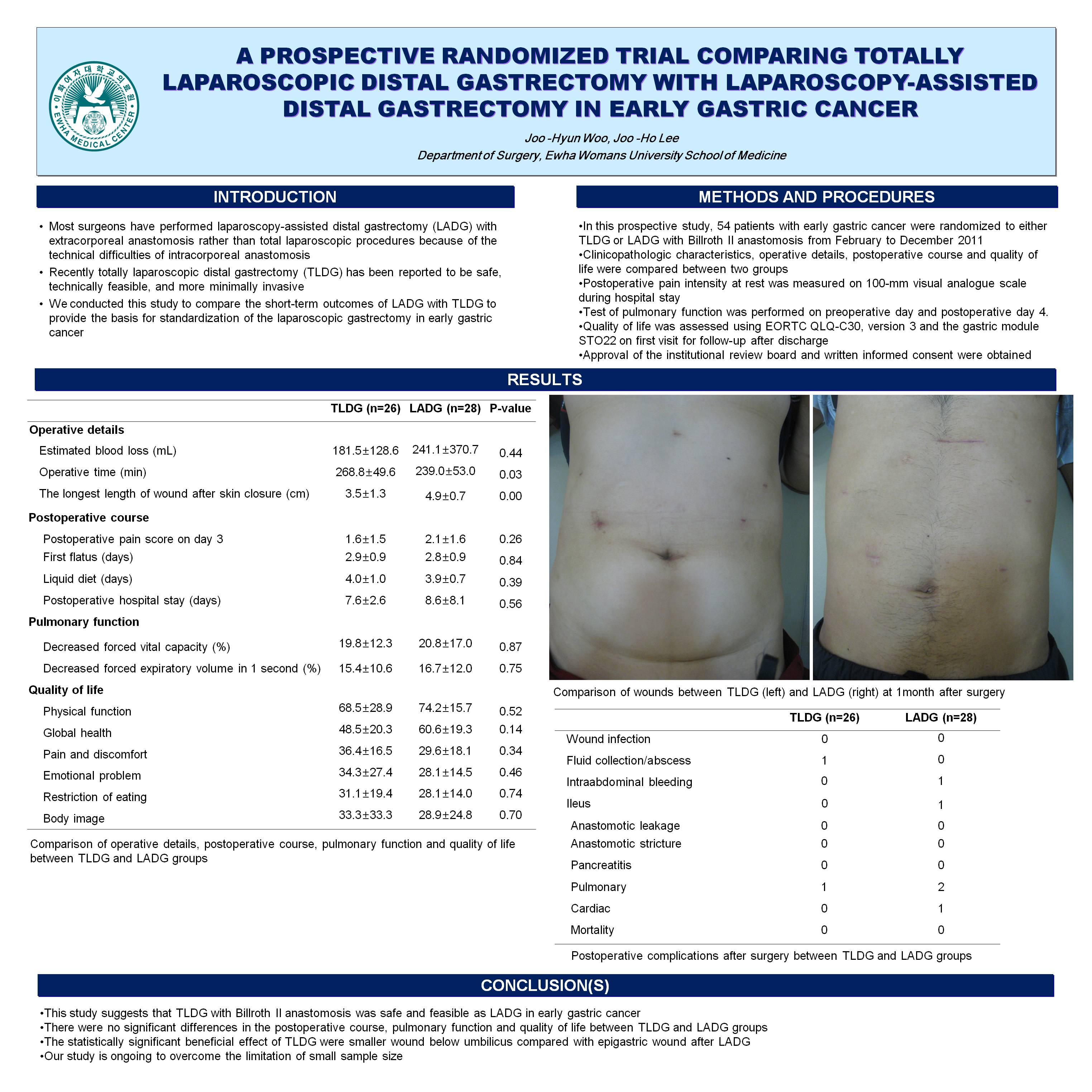
CONCLUSION(S) This study suggests that TLDG with Billroth II anastomosis was safe and feasible as LADG in early gastric cancer. The statistically significant beneficial effect of TLDG were smaller wound below umbilicus compared with epigastric wound after LADG and more healthy physical function of quality of life. Our study is ongoing to overcome the limitation of small sample size.
Session Number: Poster – Poster Presentations
Program Number: P617
View Poster