Christopher Wright, Mr, Matthew Tutton, Mr. Department of Colorectal Surgery, Colchester General Hospital
Introduction
This is the first description of primary use of biological mesh for both pelvic floor and parastomal region during APR. Poor perineal wound healing and parastomal hernias following abdominoperineal resection (APR) causes significant morbidity. The risk of parastomal hernias is up to 70% in the literature. Many authors have looked at prevention of both parastomal and pelvic floor hernias with mesh. Due to the complications of synthetic mesh there has been an interest in the use of biological mesh for both of these problems.
Method
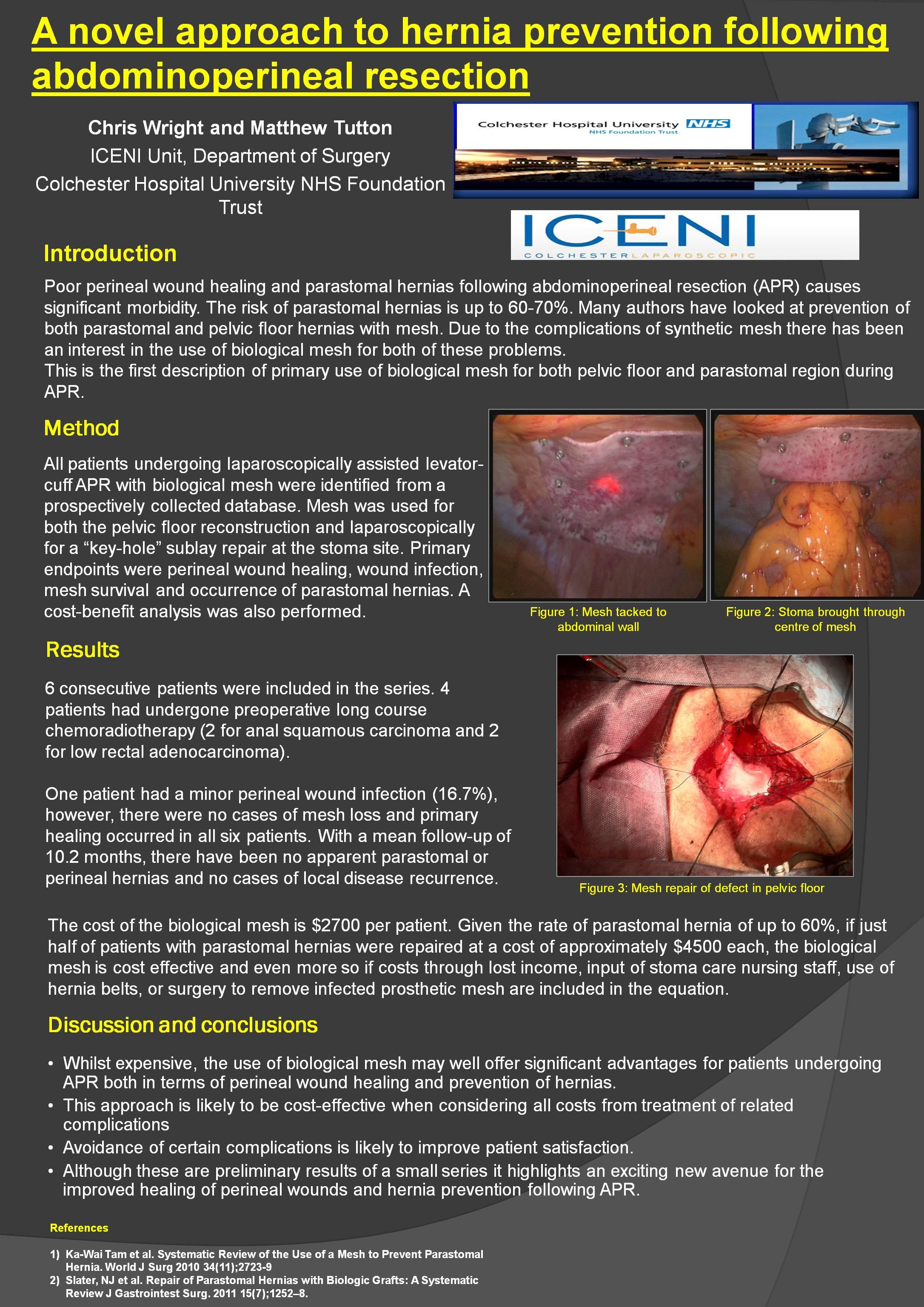
A retrospective study of all patients undergoing laparoscopically assisted levator-cuff APR with biological mesh was undertaken from a prospectively collected database. Mesh was inserted in both the pelvic floor reconstruction and laparoscopically as a “key-hole” sublay repair at the stoma site. Primary endpoints were perineal wound healing, wound infection, mesh survival and occurrence of parastomal hernias. A cost-benefit analysis was also performed.
Results
6 consecutive patients were included in the series. 4 patients had undergone preoperative long course chemoradiotherapy (2 for anal squamous carcinoma and 2 for low rectal adenocarcinoma). One patient had a perineal wound infection (16.7%), however, there were no cases of mesh loss and primary healing occurred in all six patients. With a mean follow-up of 10.2 months (+/-3.5 S.E), there have been no stoma complications, parastomal or perineal hernias and no cases of local disease recurrence. The cost of the biological mesh is $2700 per patient with very little increase in operative time for mesh placement. If just half of patients with parastomal hernias were repaired at a cost of approximately $4500, the biological mesh is cost effective and even more so if costs through lost income, input of stoma care nursing staff, use of hernia belts, or removal of infected prosthetic mesh are included in the equation.
Conclusions
Whilst expensive, the use of biological mesh may well offer significant advantages for patients undergoing APR both in terms of perineal wound healing and prevention of hernias. This approach is likely to be cost-effective when considering all costs from treatment of related complications and may improve patient satisfaction. Although these are preliminary results of a small series it highlights an exciting new approach for the improved healing of perineal wounds and hernia prevention following APR.
Session Number: Poster – Poster Presentations
Program Number: P077
View Poster