Masanori Terashima, MD PhD FACS, Masanori Tokunaga, MD, Etsuro Bando, MD PhD, Yutaka Tanizawa, MD, Taiichi Kawamura, MD PhD, Junya Kondo, MD, Yusuke Kinugasa, MD PhD, Hideyuki Kanemlto, MD, Katsuhiko Uesaka, MD PhD, Kohei Takizawa, MD, Masaki Tanak. Division of Gastric Surgery, gastrointestinal Surgery, and Endoscopy, Shizuoka Cancer Center
Introduction: Submucosal tumor (SMT) of the stomach including gastrointestinal stromal tumor (GIST) is a good candidate for minimal-invasive surgery because the tumor rarely metastasizes to lymph node. Laparoscopic partial gastrectomy using linear stapler is most popular operative procedure for this type of tumor. Actually, this procedure is very simple and even possible for single port surgery. However, delayed gastric emptying due to severe deformity of the stomach after partial gastrectomy is sometimes observed in patients with intraluminal type SMT especially located near the cardia or the pylorus. Recently, several investigators had been reported the usefulness of hybrid technology using laparoscopic and endoscopic procedure to prevent the deformity of the stomach after partial gastrectomy. Even though using this modern technology, deformity of the stomach is sometimes inevitable if the surgeons use linear staple for tumor located near the cardia or the pylorus. Therefore, we have developed a new hybrid technology to avoid the gastric deformity for intraluminal type SMT of the stomach.
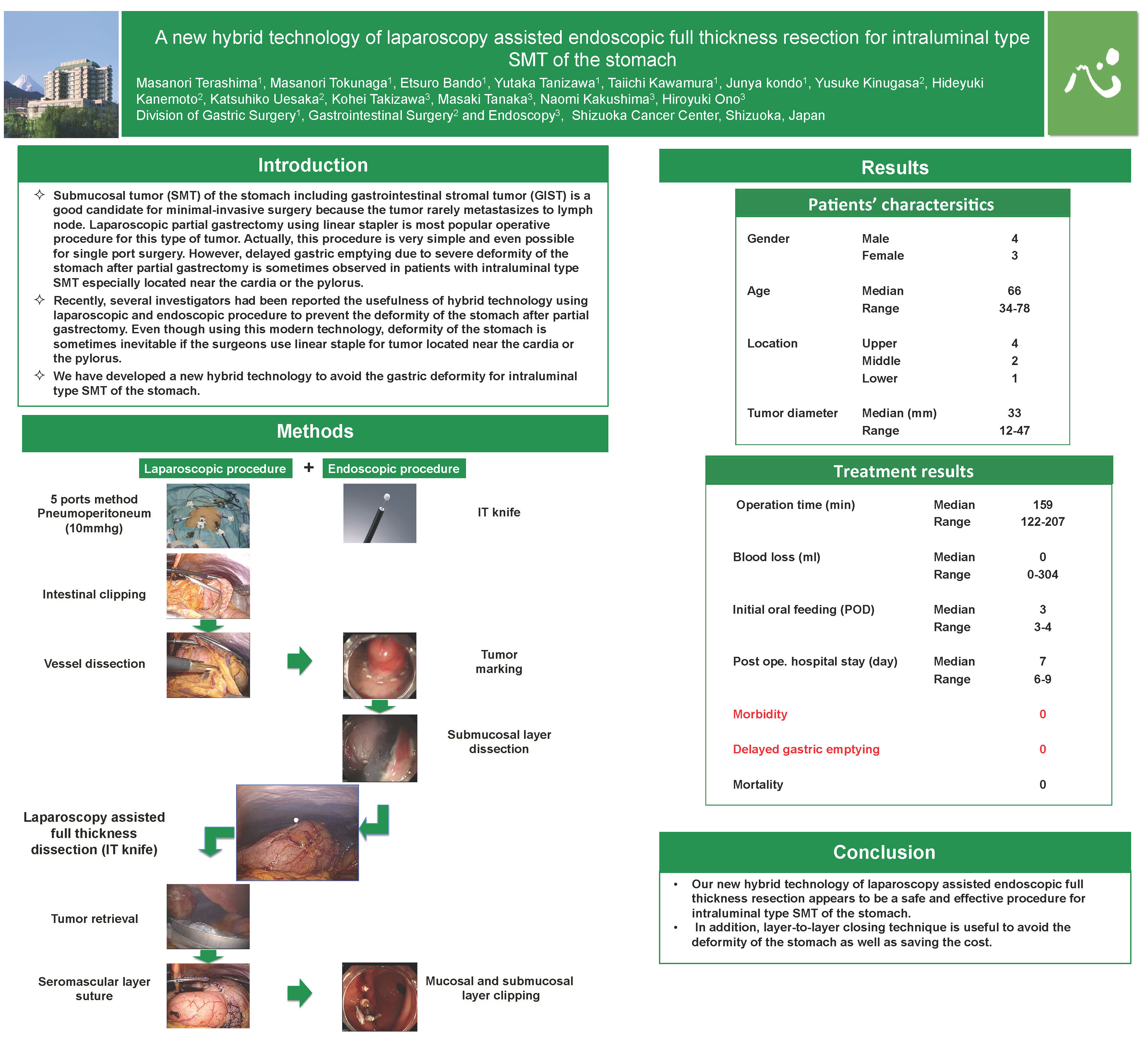
Method: Under general anesthesia, vessels around the tumor were dissected using ultrasonically activated device under usual laparoscopic procedure with 5 ports method. Mucosal and submucosal layers around the tumor were cut circumferentially using the technique of endoscopic submucosal dissection via intraluminal endoscopy. Then, full thickness of gastric wall was also dissected under intraluminal endoscope using IT knife2 under the observation and guide of laparoscope. Tumor was completely dissected circumferentially using intraluminal endoscope, and retrieved from abdominal cavity with usual laparoscopic procedure. After resection of the tumor, seromascular layer of the stomach was sutured using hand-sawn technique under laparoscope, and mucosal and submucosal layer was closed using hemostatic clip under intralluminal endoscope.
Result: From January 2010 to August 2010, this operation was performed for a total of 6 patients. There were 4 male and 2 female. The pathological diagnosis was GIST in all patients. The median operation time was 166 (122-207) min, and the median estimated blood loss was 0 (0-304) ml. Oral feeding was started at the 3rd postoperative day in all patients. The median duration of hospital stay was 7.5 (6-9) days. The postoperative course was uneventful and delayed gastric emptying was not observed in all patients.
Conclusion: Our new hybrid technology of laparoscopy assisted endoscopic full thickness resection appears to be a safe and effective procedure for intraluminal type SMT of the stomach. In addition, layer-to-layer closing technique is useful to avoid the deformity of the stomach as well as saving the cost.
Session: Poster
Program Number: P273
View Poster
{kind=link}