Subhasis Misra, MD, Alexander Fort, BA, Nestor De La Curz, MD, Alan Livingstone, MD. University of Miami
Background: Open Ivor-Lewis esophagectomy and open Transhiatal esophagectomy (THE) is known to be associated with significant morbidity and mortality. Few studies have been published comparing an open transhiatal approach and a laparoscopic transhiatal approach without a thoracoscopic port. This study assessed whether there were significant differences between the two procedures regarding specific operative and post-operative variables.
Methods: A series of 26 patients undergoing laparoscopic or open THE performed by the same surgeon for either esophageal cancer or failed myotomy following achalasia were followed prospectively. 20 patients underwent an open resection (18 male, 2 female, average age 60.4, average BMI 27.9, 18 esophageal cancer, 2 achalasia) and 6 patients underwent a laparoscopic resection (6 male, 0 female, average age 57.5, average BMI 29.1, 5 esophageal cancer, 1 achalasia).
Results: Compared to the open group, the laparoscopic group averaged a slightly longer operative time (246 vs 231 min; p = .52), less estimated blood loss (127 vs 338 mL; p = .12), less lymph nodes (LN) sampled (15 vs 22 LN; p = .07), and a shorter length of stay (LOS) (9 vs 11 days; p = .12). In regards to pain medication requirements, patients undergoing the laparoscopic procedure had lower averages in morphine PCA use (98 vs 143 mL; p = .65), Roxicet use (57 vs 77 mL; p = .66), and Toradol use (20 vs 92 mg; p = .01). Only total Toradol use proved to be statistically significant. Also, in regards to other analgesic medications, patients undergoing the open procedure required more oral analgesics to control their pain both in supplementation of their PCA and following PCA discontinuation while in the hospital. The open group had one anastomotic leak and one post-operative death while the laparoscopic group did not have either complication.
Conclusions: Early experiences with laparoscopic THE indicate that this is a safe alternative in experienced hands without any oncologic compromise. The greatest advantage is in post-operative patient comfort – the patients undergoing the laparoscopic procedure had significantly less pain medication requirements. Patients undergoing laparoscopic resection also had less blood loss during surgery and a shorter length of stay in the hospital. Our findings suggest an open approach may yield a higher number of LN harvested. Since the group was not randomized, LN numbers may have been less due to earlier preoperative staging and a case of nonmaligmant disease. LN retrieval will likely improve with a laparoscopic approach as the surgeon becomes more experienced with the procedure.
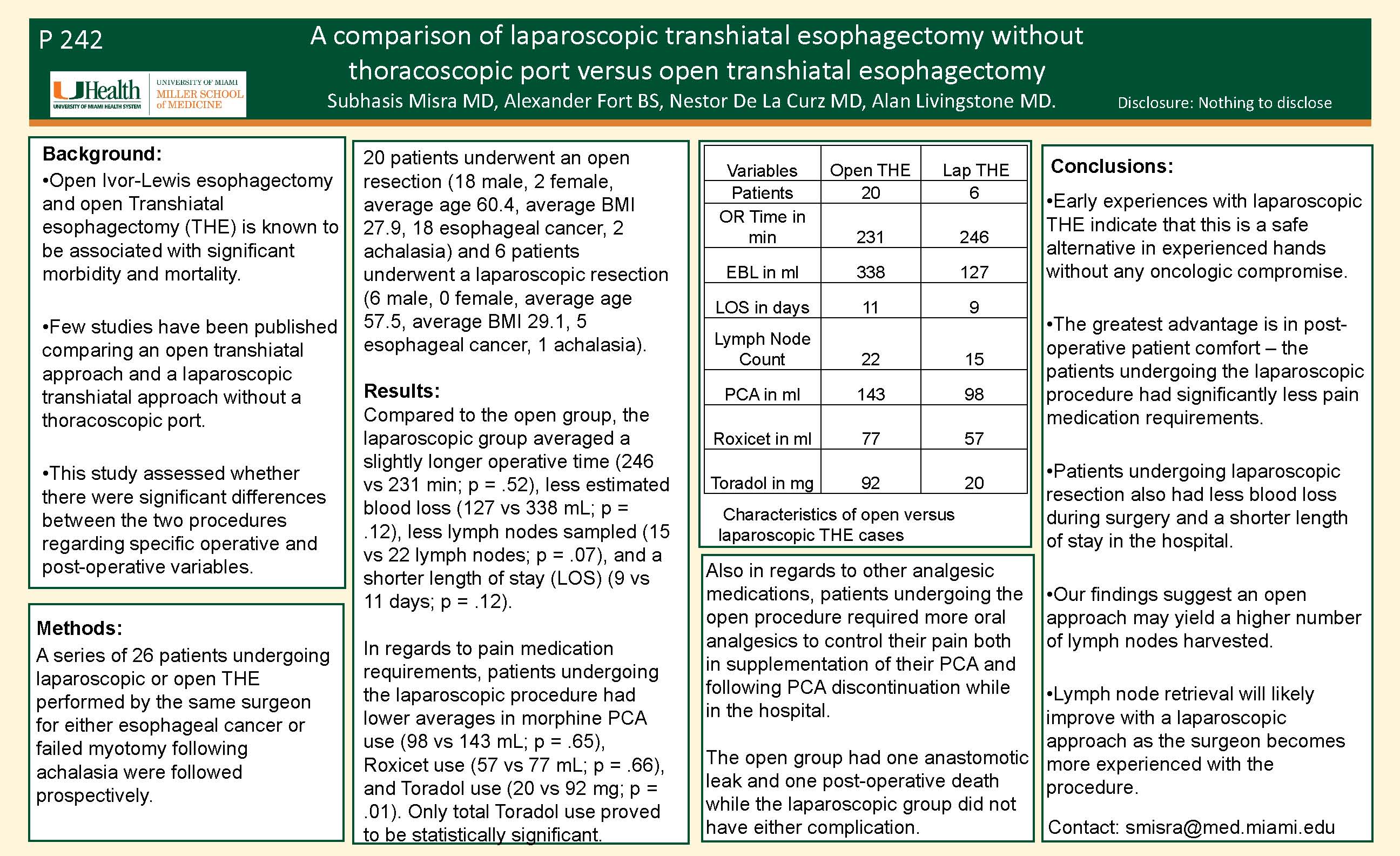
| Variables | Open THE | Lap THE |
| Patients | 20 | 6 |
| OR Time in min | 231 | 246 |
| EBL in ml | 338 | 127 |
| LOS in days | 11 | 9 |
| Lymph Node Count | 22 | 15 |
| PCA in ml | 143 | 98 |
| Roxicet in ml | 77 | 57 |
| Toradol in mg | 92 | 20 |
Session: Poster
Program Number: P242
View Poster
{kind=link}