cholecystoduodenal fistula
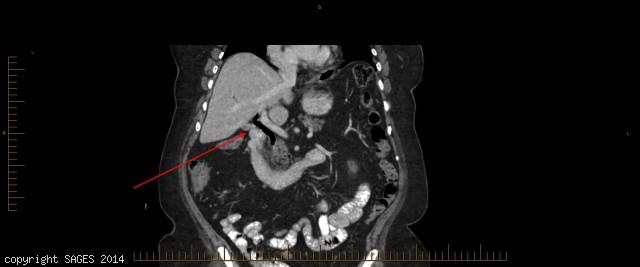
50 year old female who presented with repeated attacks of RUQ pain. CT scan showed pneumobilia and cholecystoduodenal fistula, which was confirmed intraoperatively.
Critical View

To perform a safe Laparoscopic Cholecystectomy, demonstration of the critical view following dissection of the triangle of Calot is essential. Laparoscopic view – Cystic Duct & Artery, CBD are shown.
Fundus-down Laparoscopic Cholecystectomy
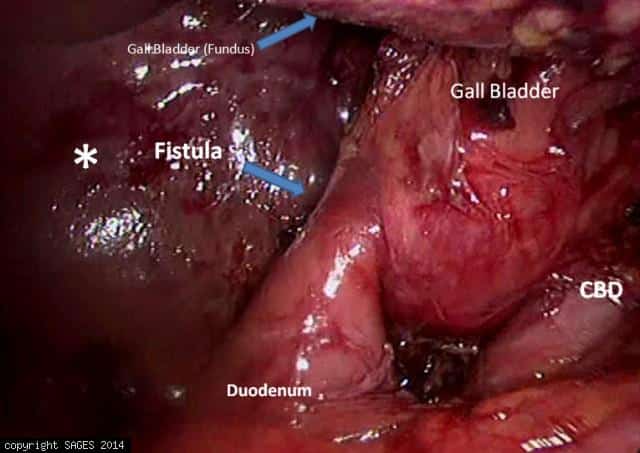
Fundus-down approach (retrograde dissection).Surgical field—Laparoscopic view of fundus-down approach. Liver(Gall bladder Bed)[asterisk]; Fistula between gall bladder neck and duodenum(arrow); fundus of gall bladder over the grasper after FDA (arrow).
Fundus-down Laparoscopic Cholecystectomy
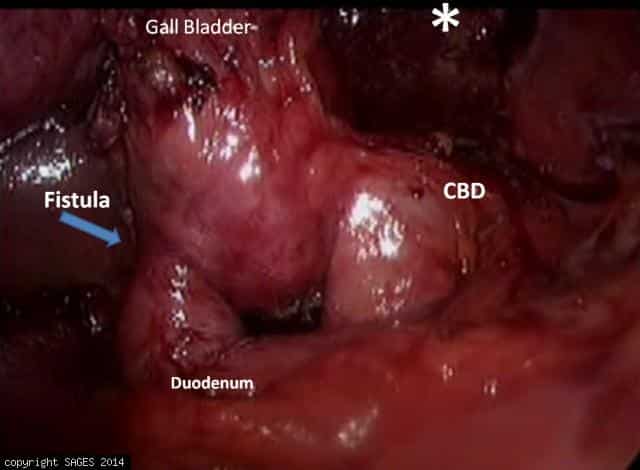
Fundus-down approach (retrograde dissection).Surgical field—Laparoscopic view of fundus-down approach. Liver(Gall bladder Bed)[asterisk]; Fistula between gall bladder neck and duodenum(arrow).
Fundus-down Laparoscopic Cholecystectomy

Fundus-down approach (retrograde dissection).Surgical field—Laparoscopic view of fundus-down approach. Liver(Gall bladder Bed)[asterisk]; Fistula between gall bladder neck and duodenum(arrow).