Veress needle
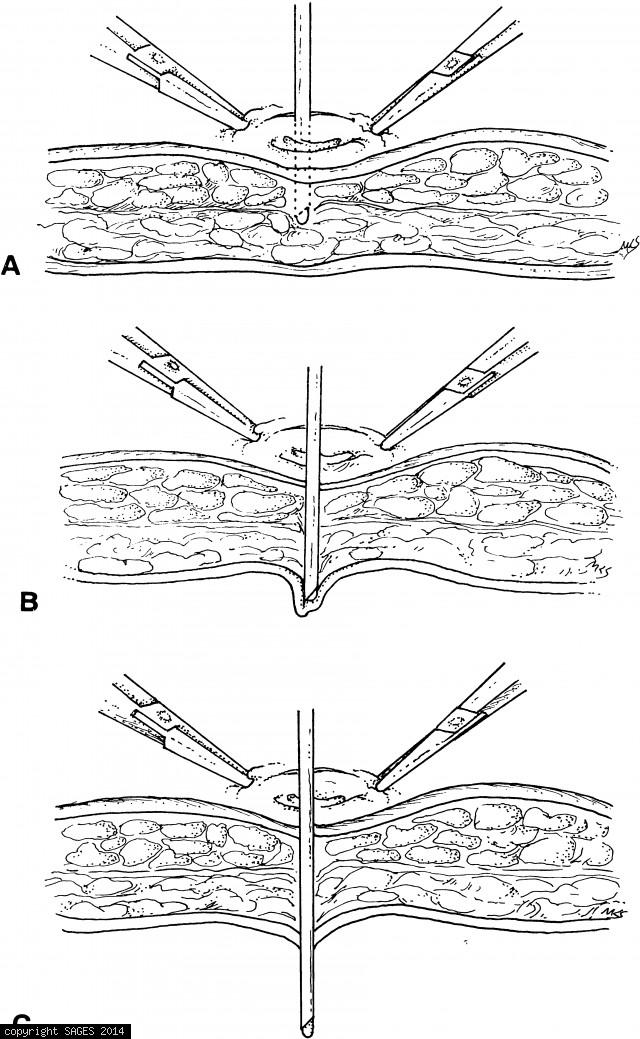
A. Veress needle inserted at umbilicus (sagittal view; the blunt tip retracts as it encounters the fascia of the linea alba). B. As the sharp edge of the needle traverses the fascia, the blunt tip springs forward into the preperitoneal space and then r
Site of Veress needle insertion at superior crease

stab incision has been made. Transverse oblique section at superior crease of umbilicus; the peritoneum is closer to the skin at the umbilicus and is more densely adherent to the umbilicus than at any other site along the abdominal wall.
Testing retractable tip of disposable Veress needl
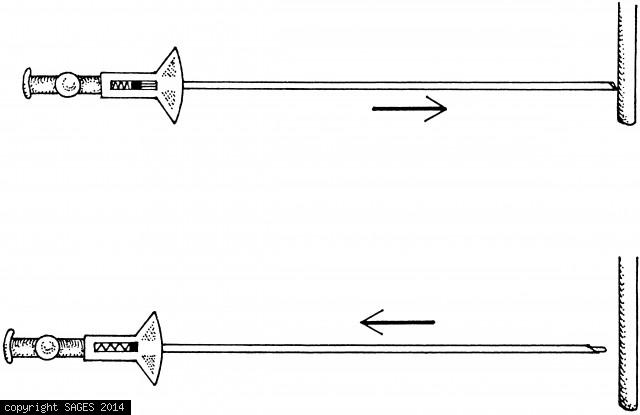
A. Blunt tip retracts as it contacts resistance (e.g., a knife handle). B. When the needle is pulled away from the point of resistance, the blunt tip springs forward and protrudes in front of the sharp edge of the needle.
Insufflator testing.

With the insufflation tubing kinked, the intraabdominal pressure should rapidly rise (e.g., 30mmHg), thereby exceeding the preset 15mmHg pressure set point. The flow of CO2 should immediately cease (0 L/min) and an alarm should sound.
Insufflator testing

With insufflator tubing open (i.e., not connected to Veress needle) and flow rate set at 6 L/min, the intra-abdominal pressure reading obtained through the open insufflation line should be 0mmHg