Chao Li, MD, Francesco Carli, MD MPhil, Patrick Charlebois, MD, Barry Stein, MD, Alexander S Liberman, MD, Berson Augustin, BSc, Pepa Kaneva, MSc, Ann Gamsa, PhD, Do J Kim, MSc, Gerald M Fried, MD, Melina C Vassiliou, MD MEd, Liane S Feldman, MD. McGill Unversity Health Centre
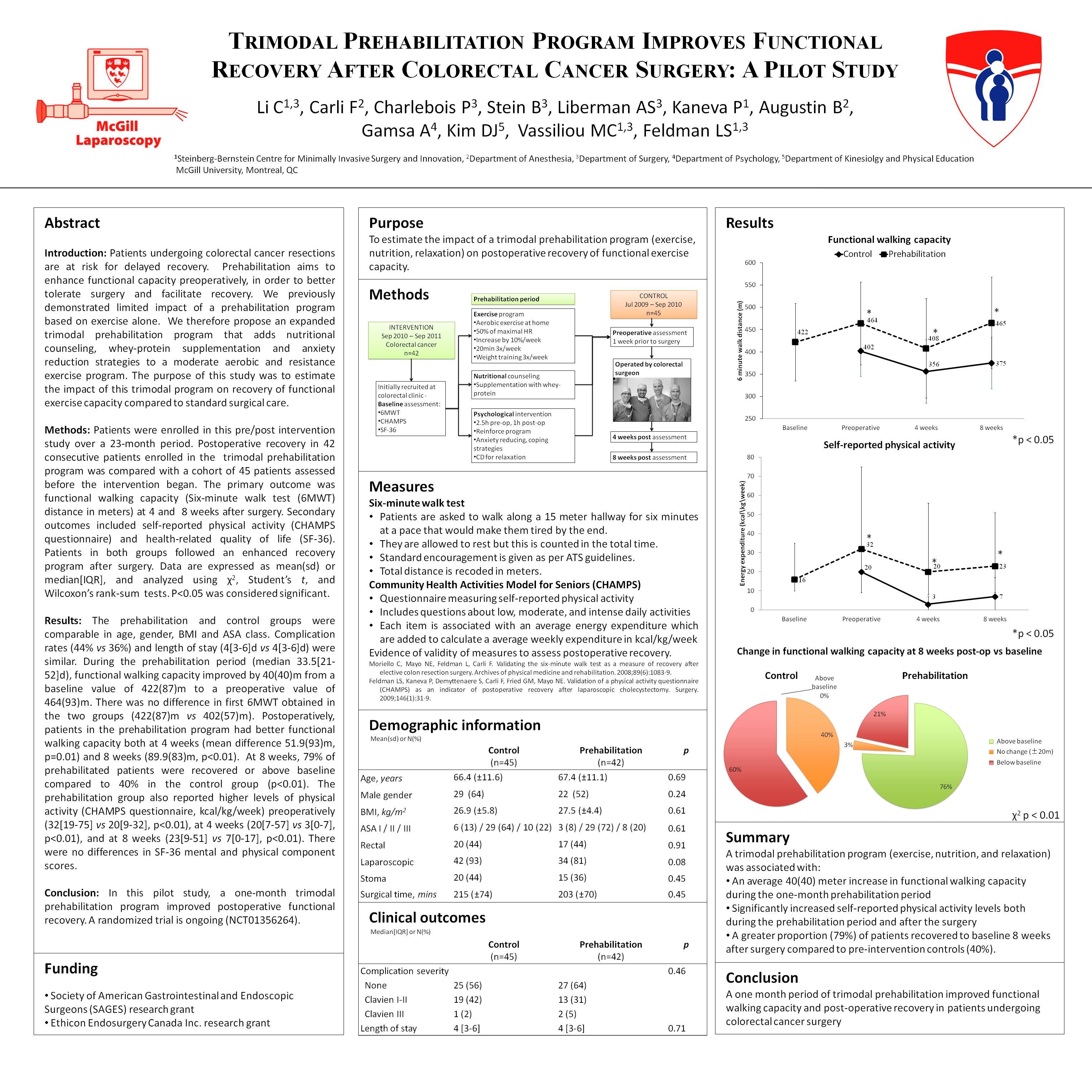
Introduction: Patients undergoing colorectal cancer resections are at risk for delayed recovery. Prehabilitation aims to enhance functional capacity preoperatively in order to better tolerate surgery and accelerate recovery. We previously demonstrated the limited impact of a prehabilitation program based on exercise alone. We therefore propose an expanded trimodal prehabilitation program that adds nutritional counseling, whey-protein supplementation and anxiety reduction strategies to a moderate aerobic and resistance exercise program. The purpose of this study was to estimate the impact of this trimodal program on recovery of functional exercise capacity compared to standard surgical care.
Methods: Between September 2010 and June 2011, 42 consecutive patients with colorectal cancer were enrolled in the trimodal prehabilitation program. The primary outcome was functional walking capacity as measured by the Six-minute walk test (6MWT) at baseline and preoperatively after the 4-week prehabilitation program, then at 4 and 8 weeks after surgery. Secondary outcomes included self-reported physical activity (CHAMPS questionnaire) and health-related quality of life (SF-36). Comparison was made to a similarly assessed cohort of 45 consecutive patients with colorectal cancer admitted between July 2009 and Sep 2010 receiving standard care. Patients in both groups followed an enhanced recovery program after surgery. Data are expressed as mean(SD) or median[IQR], and analyzed using χ2, Student’s t, and Wilcoxon’s rank-sum tests.
Results: The prehabilitation and control groups were comparable in age, gender, BMI and ASA class. More patients in the control group underwent laparoscopic colon resection (93% vs 81%). Complication rates (44% vs 36%) and length of stay (4[3-6]d vs 4[3-6]d) were not significantly different. During the prehabilitation period (median 33.5[21-45]d), functional walking capacity improved by 40(40) meters from a baseline value of 422(87)m to a preoperative value of 464(93)m. There was no difference between the baseline 6MWT in the prehabilitation group and the first value obtained in the control group immediately before surgery (422(87)m vs 402(57)m). Postoperatively, patients in the prehabilitation program had better functional walking capacity compared to control both at 4 weeks (408(112)m vs 356(71m), p=0.01) and 8 weeks (465(103)m vs 375(58)m, p<0.01). At 8 weeks, 75% of prehabilitated patients were improved from their baseline compared to 0% in the control group (p<0.01). The prehabilitation group also reported higher levels of physical activity (CHAMPS questionnaire, kcal/kg/week) preoperatively (32[19-75] vs 20[9-32], p<0.01), at 4 weeks (20[7-57] vs 3[0-7], p<0.01), and at 8 weeks (23[9-51] vs 7[0-17], p<0.01). There were no differences in SF-36 mental and physical component scores.
Conclusion: In this pilot project, a one-month trimodal prehabilitation program resulted in increases in functional walking capacity and self-reported physical activity in patients awaiting resection for colorectal cancer. Compared to a previously assessed control group, prehabilitation was associated with improved functional walking capacity preoperatively and substantial improvement in walking capacity after surgery. Moreover, increases in self-reported physical activity were maintained in the postoperative period. Prehabilitation may be a valuable component of an enhanced recovery program.
Session Number: PDIST – Posters of Distinction
Program Number: P001
View Poster