Hideaki Tsutsumida, MD, Mitsunobu Uto, MD, Toshiro Kamimura, MD. Department of Surgery, Keiaikai Kamimura Hospital
Introduction:
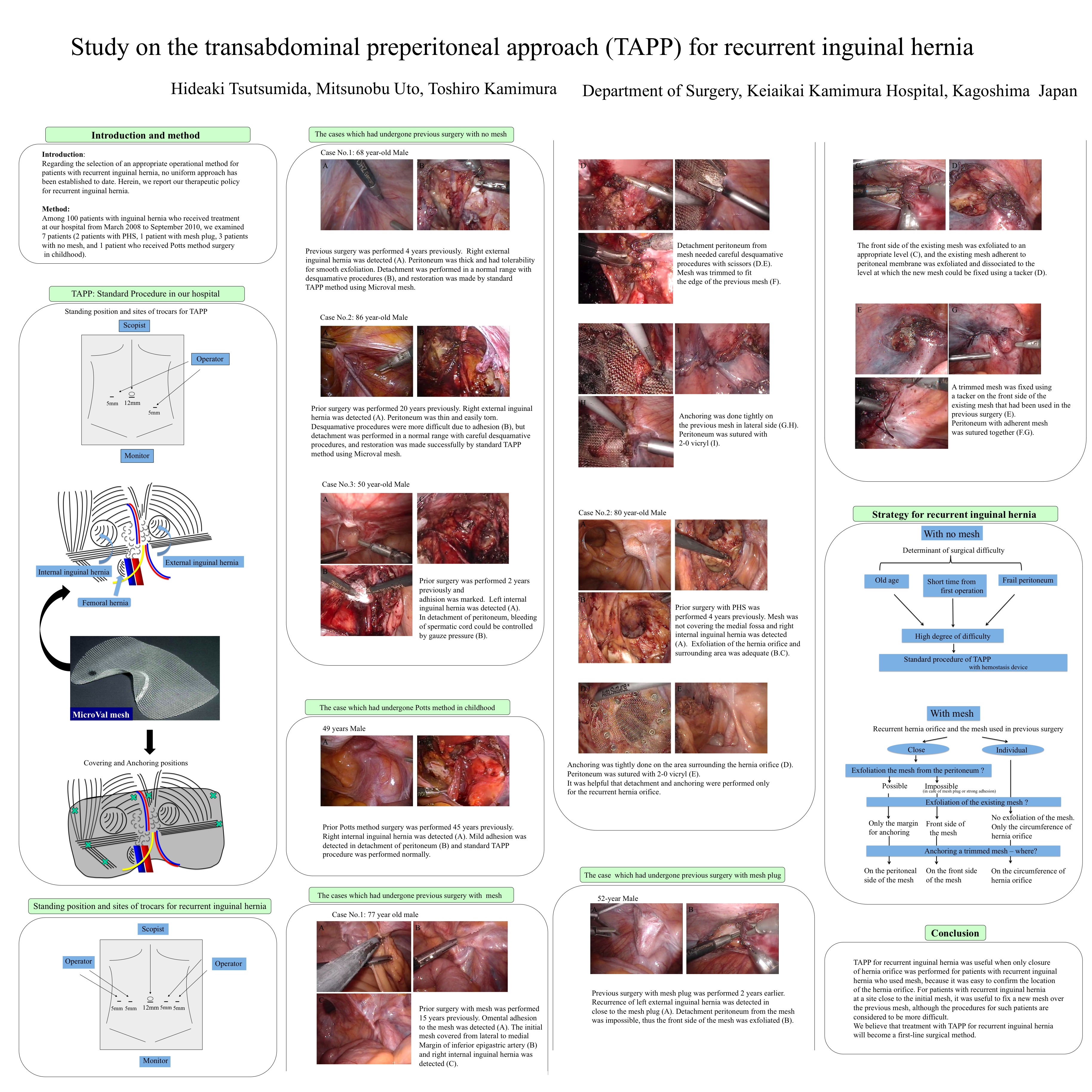
Regarding the selection of an appropriate operational method for patients with recurrent inguinal hernia, no uniform approach has been established to date. Herein, we report our therapeutic policy for recurrent inguinal hernia.
Method:
Among 100 patients with inguinal hernia who received treatment at our hospital from March 2008 to September 2010, we examined 6 patients (3 patients with PHS, 1 patient with mesh plug, 1 patient with no mesh, and 1 patient with experience of Potts method in childhood).
Result:
We performed the Transabdominal Preperitoneal Approach (TAPP) for each of the 6 patients. In the 3 patients who had undergone previous surgery with no mesh, desquamative procedures were more difficult due to adhesion, but detachment was performed in a normal range with careful desquamative procedures, and restoration was made successively using micromesh. The average operation time was 115 min., and the postoperative course was favorable with no complication of hemorrhage. In the 3 patients who had undergone previous surgery with mesh, proline mesh, for which trimming was performed along the shape of hernia orifice, was fixed around the hernia orifice using a tacker for reinforcement. In the patients with recurrent hernia who had undergone previous surgery with a mesh plug, and in whom the hernia orifice had been confirmed to close with the mesh, it was considered to be impossible to exfoliate the mesh from the peritoneal membrane, and thus the front side of the mesh was exfoliated to an appropriate level, and the mesh adherent to peritoneal membrane was exfoliated and dissociated to the level at which the mesh could be fixed using a tacker. A trimmed mesh was fixed using a tacker on the front side of the mesh that had been used in the previous surgery. Regarding the 3 patients with recurrent inguinal hernia after the use of mesh, the average operation time was 130 min. and the postoperative course was favorable with no complications.
Conclusion:
TAPP for recurrent inguinal hernia was useful when only closure of hernia orifice was performed for patients with recurrent inguinal hernia who used mesh, because it was easy to confirm the location of the hernia orifice. For patients with recurrent inguinal hernia at a site close to the mesh, it was useful to fix a new mesh over the previous mesh, although the procedures for such patients are considered to be more difficult. We believe that treatment with TAPP for recurrent inguinal hernia will become a first-line surgical method.
Session: Poster
Program Number: P311
View Poster
{kind=link}