Introduction: Hand-assisted laparoscopic surgery has been recognized as a safe laparoscopic operative procedure for gastrointestinal malignancies. Although laparoscopic procedure has recently been applied for esophageal cancer, open surgery still remains the standard operative procedure. To overcome the technical difficulty of video-assisted esophagectomy, we applied hand-assisted surgery in VATS esophagectomy. The aim of this study is to assess the feasibility of safety and clinical outcomes of the hand assisted thoracoscopic surgery (HATS) in esophagectomy by reviewing our experiences.
Methods: Since 1996, we started applying VATS esophagectomy for selected thoracic esophageal cancer cases. From 1998, we introduced HATS for almost all operative esophageal cancer cases including advanced cancer as a standard procedure at our institute. For medical high risk patients and superficial cancer cases, mediastinoscope-assisted transhiatal esophagectomy was utilized. By applying these laparoscopic procedures, the overall percentage of the video assisted operations reached 99% (135/137cases). The procedure of HATS esophagectomy is as follows: to assist the surgeon’s operative procedure, an assistant surgeon inserts his left hand into the right thoracic cavity through a small incision in the upper abdomen. Retraction of the lung and trachea are done manually with the hand of the assistant. The abdominal incision is then used for hand assisted laparoscopic surgery (HALS).
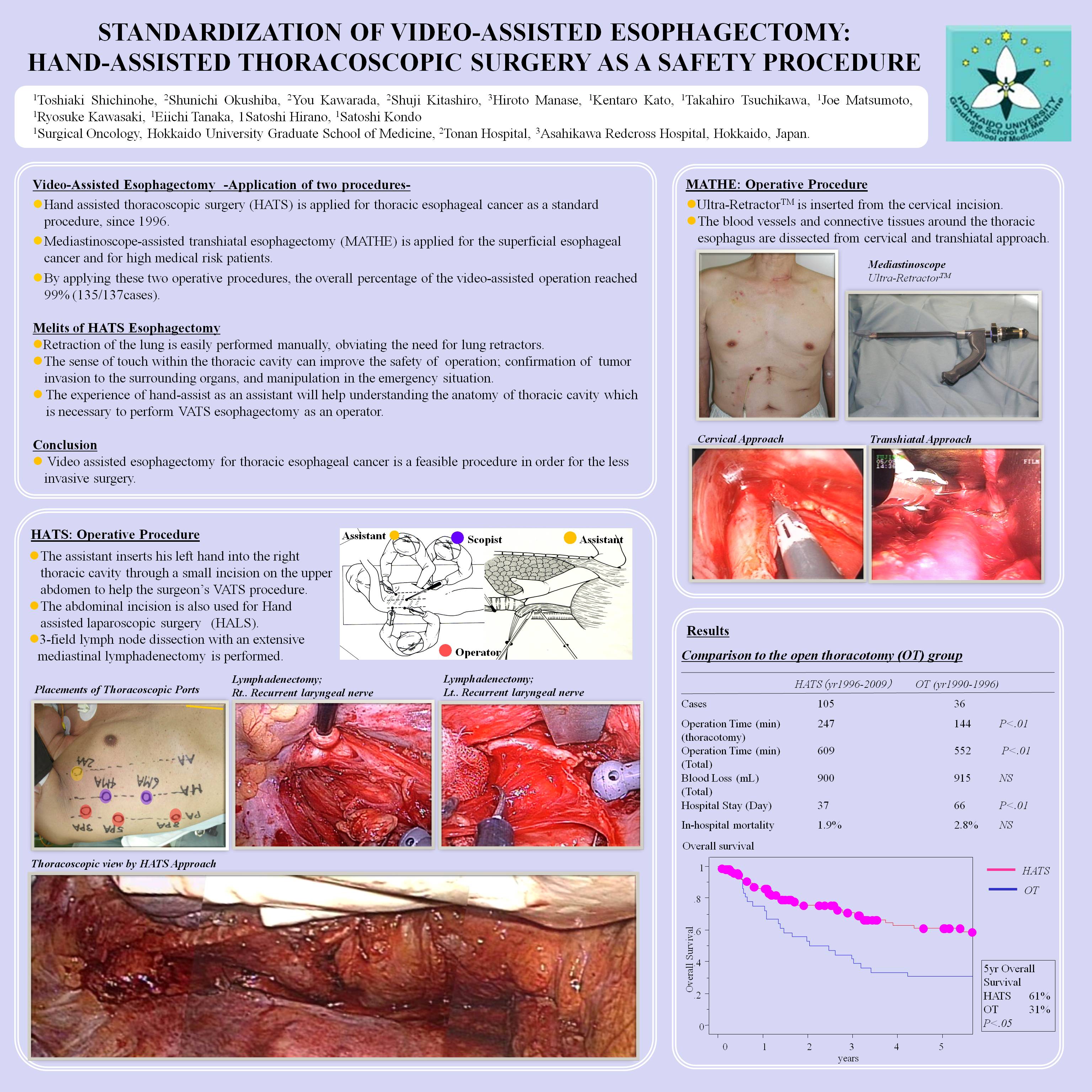
Results: We experienced 105 cases of video assisted esophagectomy (VATS group). The VATS group was compared to the radical open thoracotomy group (36cases from 1990 to 1996). The results of compared operation factors (blood loss, operation time, the number of dissected mediastinal lymph nodes, hospital stay) showed prolonged operation time and shorten hospital stay in the VATS group. In-hospital mortality rate of VATS esophagectomy was 1.9% (2/105cases). The average of 5-year survival rate of HATS group was marked by a prolonged overall survival compared to the open thoracotomy group (61% vs. 31%).
Conclusion: The advantage of HATS is the gentle retraction of the lung from the caudal side of the thorax, obviating the need for lung retractors. Moreover, this procedure allows the surgeon’s hand to use its sense of touch within the thoracic cavity, which can confirm if the tumor has invaded the surrounding organs such as the trachea. Moreover, the experience of hand-assist as an assistant will help understanding the anatomy of thoracic cavity which is necessary to perform VATS esophagectomy as an operator. Our experiences show that HATS results are at least similar or sometimes better. HATS therefore has the potential to become the standard procedure for VATS esophagectomy.
Session: Poster
Program Number: P329

{kind=link}