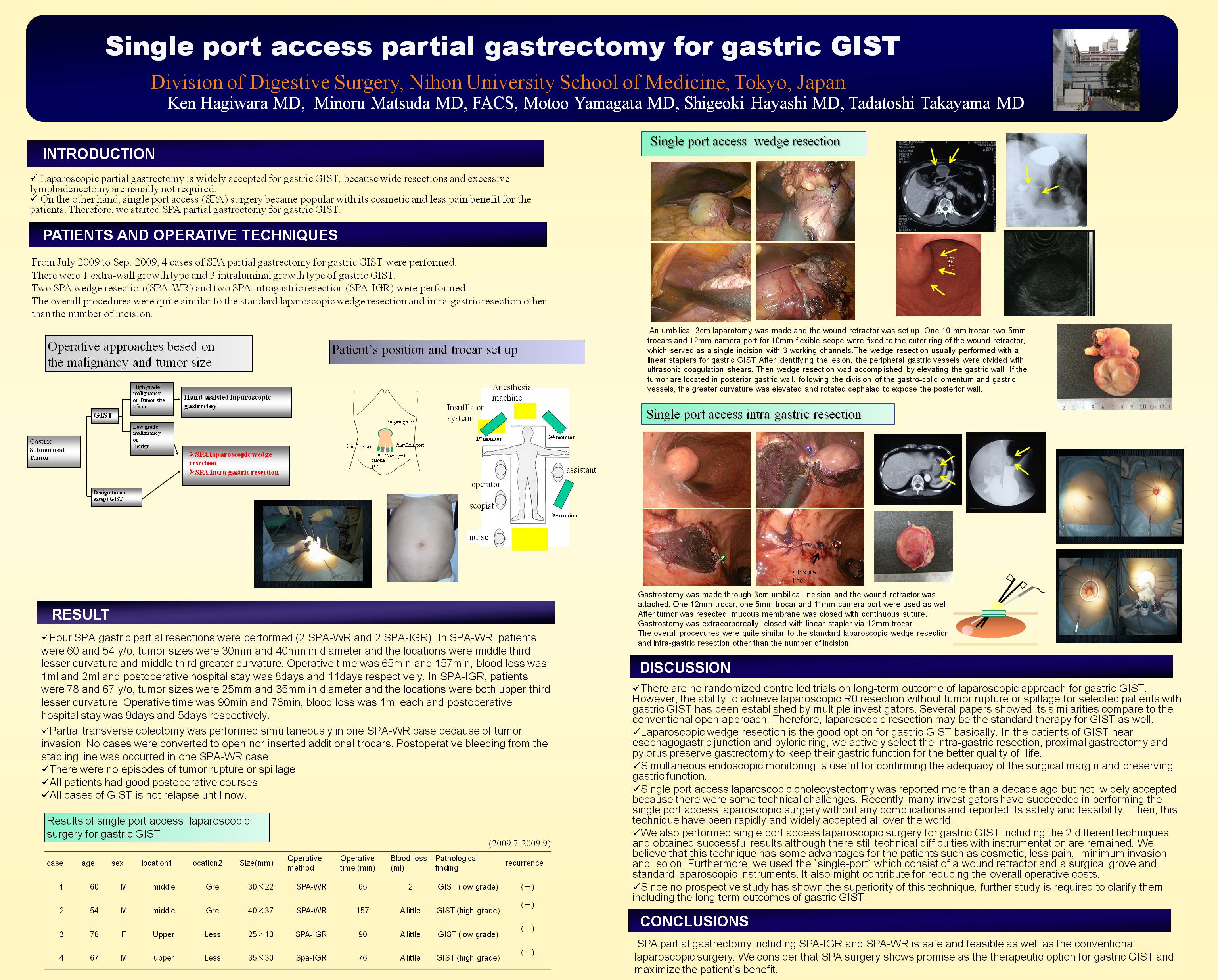
Introduction: Laparoscopic partial gastrectomy is widely accepted for gastric GIST, because wide resections and excessive lymphadenectomy are usually not required. On the other hand, single port access (SPA) surgery became popular with its cosmetic and less pain benefit for the patients. Therefore, we started SPA partial gastrectomy for gastric GIST.
Patients and Operative technique: From July 2009 to Sep. 2009, 4 cases of SPA partial gastrectomy for gastric GIST were performed. There were 1 extra-wall growth type and 3 intraluminal growth type of gastric GIST. Two SPA wedge resection (SPA-WR) were performed and two SPA intragastric resection (SPA-IGR) were performed.
In SPA-WR, an umbilical 3cm laparotomy was made and the wound retractor was set up. One 10 mm trocar, two 5mm trocars and 12mm camera port for 10mm flexible scope were fixed to the outer ring of the wound retractor, which served as single incision with 3 working channels.
In SPA-IGR, the gastrostomy was made through 3cm umbilical incision and the wound retractor was attached. One 12mm trocar, one 5mm trocar and 12mm camera port were used as well. Gastrostomy was closed with linear stapler extracorporeally.
The overall procedures were quite similar to standard laparoscopic wedge resection and intra-gastric resection other than the number of incision.
Results: Four SPA gastric partial resections were performed (2 SPA-WR and 2 SPA-IGR). In SPA-WR, patients were 60 and 54 y/o, tumor size were 30mm and 40mm in diameter, location were middle third lesser curvature and middle third greater curvature. Operative time was 65min and 157min, blood loss was 1ml and 2ml and postoperative hospital stay was 8days and 11days respectively. In SPA-IGR, patients were 78 and 67 y/o, tumor size were 25mm and 35mm in diameter and locations were both upper third lesser curvature. Operative time was 90min and 76min, blood loss was 1ml each and postoperative hospital stay was 9days and 5days respectively.
Partial transverse colectomy was performed simultaneously in one SPA-WR case because of tumor invasion. No cases were converted to open nor inserted additional trocars. Postoperative bleeding from the stapling line was occurred in one SPA-WR case.
Conclusions: SPA partial gastrectomy including SPA-IGR and SPA-WR is safe and feasible as well as the conventional laparoscopic surgery. We consider that SPA surgery shows promise as the therapeutic option for gastric GIST and maximize the patient’s benefit.
Session: Poster
Program Number: P323

{kind=link}