Chris G Smith, Dr, Balpreet Brar, Dr, Fatima Haggar, Ms, Joseph Mamazza, Dr, Robert Dent, Dr, Jean Denis Yelle, Dr, Husein Moloo, Dr, Isabelle Raiche, Dr. the Ottawa Hospital
INTRODUCTION: The role of prophylactic cholecystectomy and the usefulness of preoperative ultrasound in patients undergoing bariatric surgery is unclear. The objective of this study was to examine the rates of laparoscopic cholecystectomy in patients participating in a weight loss program and to identify risk factors for the development of symptomatic gallstones requiring cholecystectomy.
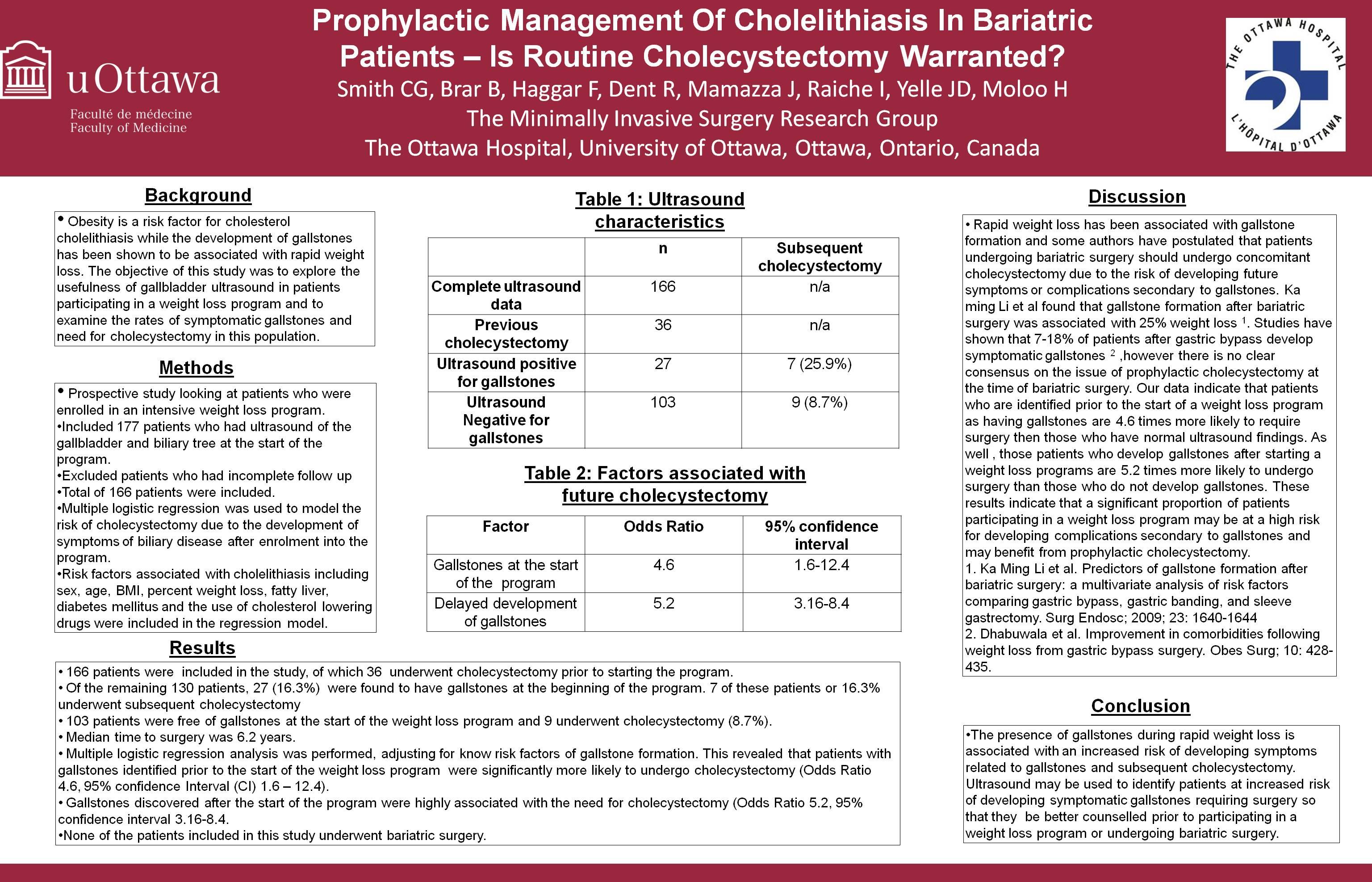
METHODS AND PROCEDURES: We prospectively studied 176 (97 females and 33 males) consecutive bariatric patients who were enrolled in an intensive weight loss program. Data from 166 patients who had a transabdominal ultrasound on week 1 of the program were analysed. Logistic regression was used to model the risk of laparoscopic cholecystectomy due to development of symptoms of biliary disease after enrolment into the program. Risk factors associated with cholelithiasis including, sex, age, BMI, % weight loss, fatty liver, diabetes mellitus and cholesterol lowering drugs were included in the regression model.
RESULTS: Gallbladder disease, as indicated by presence of gallstones on ultrasound, or previous cholecystectomy, were found in 16.3% (n=27) and 21.7% (n=36) of patients, respectively. Of the 27 who had positive ultrasound findings, 25.9 % (n=7) developed delayed symptoms related to biliary disease and underwent laparoscopic cholecystectomy. In contrast, of the 105 patients who had a negative ultrasound, 8.6% (n=9) underwent cholecystectomy. Median time to surgery was 6.2 years (interquartile range: 8.75 years). There were no post-operative complications due to cholecystectomy. Logistic regression analysis, adjusted for known risk factors of gallstones formation, revealed that patients with identified gallstones were significantly more likely to undergo laparoscopic cholecystectomy compared with those with no gallstones at the start of the program (Odds Ratio 4.6, 95% confidence interval (CI) 1.6–12.4, p-value=0.003). Discovery of cholelithiasis after starting the program was highly associated with the development of symptoms requiring cholecystectomy (Odds Ratio 5.2, 95% confidence interval (CI) 3.16–8.4, p-value<0.001).
CONCLUSION: The presence of gallstones during rapid weight loss is associated with an increased risk of developing symptoms requiring cholecystectomy. Routine preoperative ultrasound and concomitant cholecystectomy at the time of gastric bypass surgery may be indicated given this increased risk. However, the value of prophylactic cholecystectomy in the absence of symptomatic gallstones has yet to be demonstrated.
Session Number: Poster – Poster Presentations
Program Number: P446
View Poster