Isabelle Raiche, MD FRCSC, Fatima Haggar, MPH, Joseph Mamazza, MDCM FRCSC, Husein Moloo, MD FRCSC MSc, Guillaume Martel, MD FRCSC, Eric C Poulin, MD MSc FRCS C, James Masters, MD, Christopher Smith, MD FRCSC, Balpreet Brar, MD FRCSC. The Minimally Invasive Surgery Research Group, The Ottawa Hospital, University of Ottawa
Background: The elderly population often presents an increased surgical risk. The potential risk of surgical complications is always balanced against the risk of the primary disease. Paraesophageal hernias in the elderly present a unique challenge to the clinicians. The aim of this study was to 1) compare the short-term postoperative outcomes between the different surgical approaches (laparoscopy, laparotomy and thoracotomy) for paraesophageal hernia (PEH) repair in elderly patients; and 2) evaluate the short-term postoperative outcomes following emergency and elective PEH procedures in elderly patients.
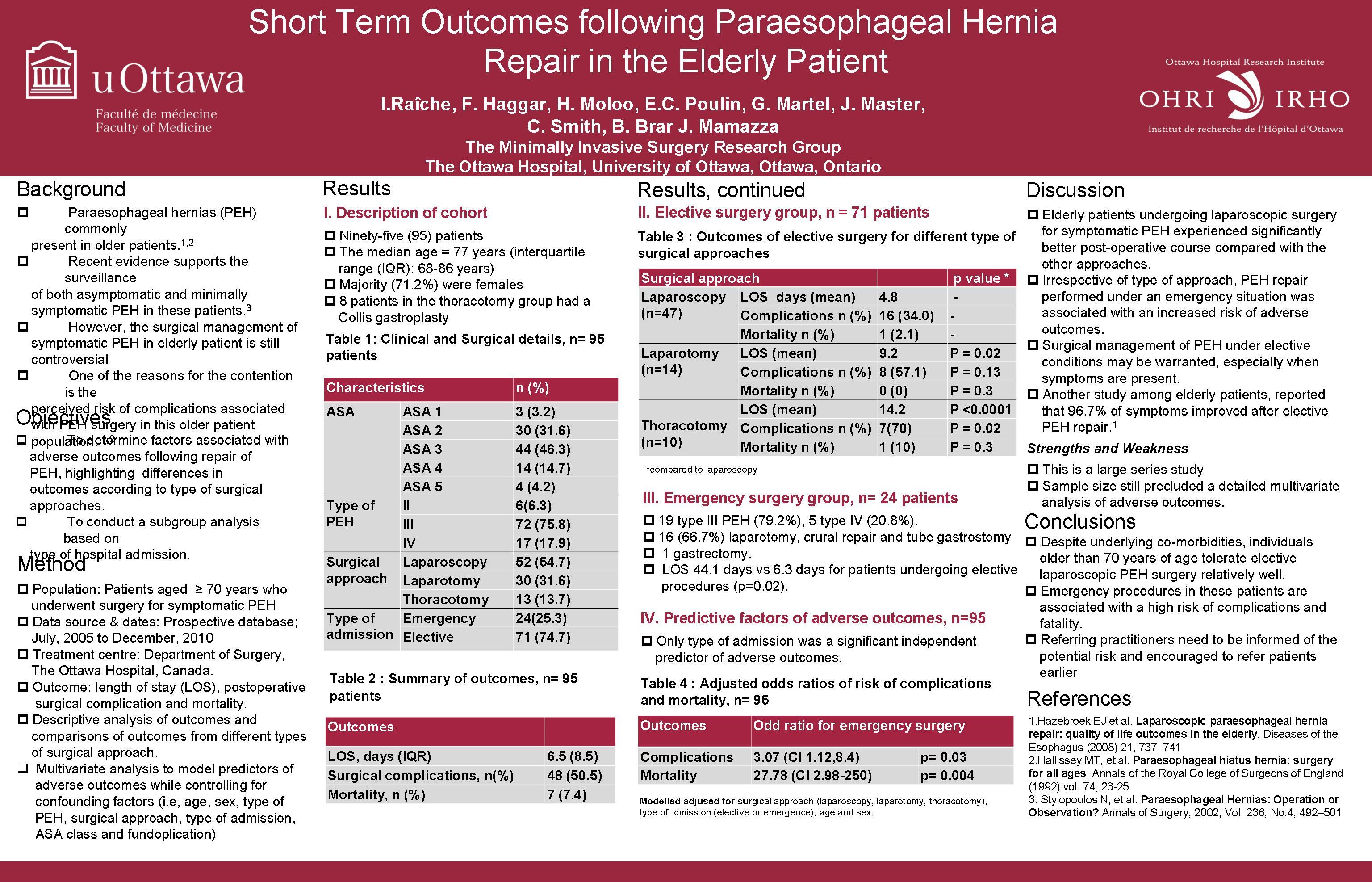
Methods: Data was obtained on patients 70 years of age or older who underwent PEH repair from a prospective database. This database included patients who underwent surgical hernia repair by laparoscopy, laparotomy or thoracotomy between July 2005 and December 2010 at a single academic center. The surgical approach was left to the surgeon discretion. Length of stay (LOS), postoperative morbidity and mortality were analysed.
Results: Ninety-five patients (27 males, 68 females) with a median age of 77 years (interquartile range, IQR: 9 years) undergoing laparoscopy (n=52, 54.7%), laparotomy (n=30, 31.6%) and thoracotomy (n=13, 13.7%) were included. In the thoracotomy group, 8 patients had a Collis gastroplasty. A majority of included patients had ASA score of II (31.6%), III (46.3%) or IV (14.7%). The most frequent diagnosis was type III PEH (n=72, 75.8%), 17 patients had type IV (17.9%) and 6 patients had type II (6.3%).
In the patients undergoing elective surgery (n=71, 74.7%), the median LOS was 6.0 days (IQR: 5 days). For this group, the median LOS for patients undergoing laparoscopy was 4.8 days, which was significantly shorter than for patients undergoing laparotomy (9.2 days, p=0.02) and thoracotomy (14.2 days, p=<0.0001). The post-operative complication rate for the laparoscopy group was 34.0% (n=16), 57.1% for the laparotomy group (n=8) and 70.0%for the thoracotomy group (n=7); the difference was statistically significant only between the thoracotomy group and the laparoscopy group (p=0.02). The overall mortality rate was 2.8% (n=2) without significant difference between the approach.
Twenty-five percent of the cases (n=24) were emergencies, 19 patients for type III PEH (79.2%) and 5 patients for type IV (20.8%). The most frequent procedure performed was a laparotomy, crural repair and tube gastrostomy (n=16, 66.7%). Three patients had a fundoplication (12.5%). Only one patient needed a gastrectomy. Patients undergoing emergency procedures on average stayed in hospital significantly longer than patients undergoing elective procedures (6.3 vs. 44.1 days, p=0.02). Elderly patients undergoing emergency PEH surgery experienced 3 times higher odds of postoperative complications (odds ratio (OR) 3.13, 95% confidence interval (CI); 1.16, 8.47 , p= 0.025) and nine (9) times higher odds of death (OR 9,09, 95% CI;1.63, 50 p=0.012) compared with those undergoing an elective procedure.
Conclusions: Despite underlying comorbidities, individuals older than 70 years of age tolerate elective laparoscopic PEH surgery relatively well. Emergency procedures for PEH are associated with an increased risk of serious adverse events or fatality. Referring practitioners need to be informed of the potential risk and encouraged to refer patients earlier.
Session Number: Poster – Poster Presentations
Program Number: P248
View Poster