B Pellini, MD, S Smith, MD, B O’connell, MD, I Daoud, MD FACS. St Francis Hospital and Medical Center, Hartford, CT
Introduction
While a number of studies have demonstrated the feasibility and early outcomes pertaining to single incision laparoscopic (SILS) cholecystectomy there is very limited published data concerning use of routine cholangiography during this procedure. Presented is the initial outpatient elective operative experience of a single surgeon’s SILS cholecystectomy with routine cholangiogram.
Methods
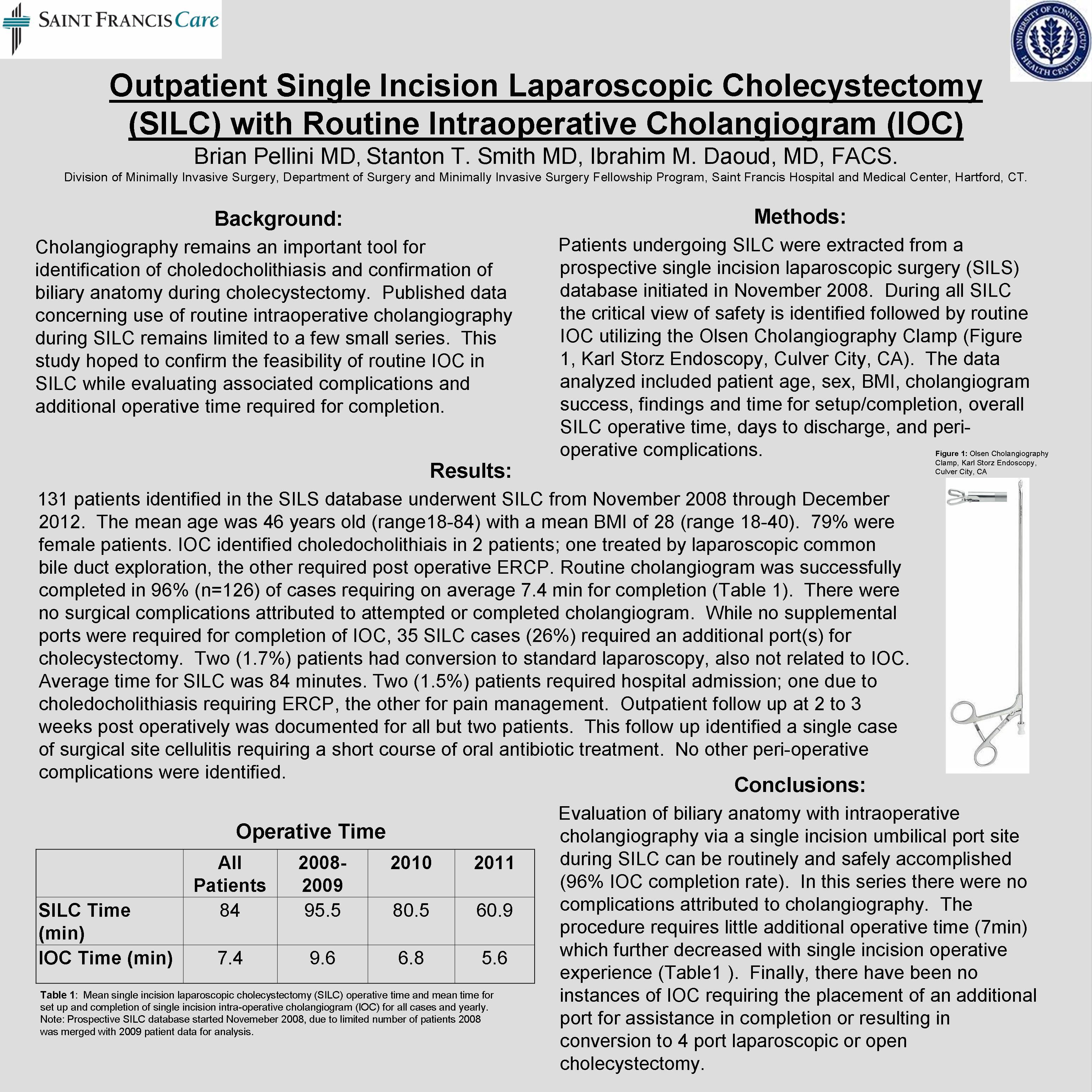
Data was gathered from a prospectively maintained single incision laparoscopic database consisting of a single surgeons experience from a community teaching hospital. All SILS cholecystectomy operations were then extracted from this database and analyzed for descriptive statistical analysis. As a general surgical approach in this practice, routine identification of the critical view of safety followed by intraoperative cholangiogram using an Olsen Cholangiogram Clamp is attempted for all SILS cholecystectomy.
Results
SILS patient data was analyzed from November 2008 through May 2011. 112 patients identified in the SILS database underwent cholecystectomy during this time. The average age was 46.2 years old (range18-84) with an average BMI of 27.7, and 78% were female patients. Routine cholangiogram was successfully completed in 95.5% of these cases (n=107), which required on average an additional 7min of operative time to the case. There were no surgical complications identified attributed either to an attempted or completed cholangiogram. While no additional ports were required specifically to perform cholangiogram, at least a single additional port was required for cholecystectomy in 35 patients (31%). There were no open conversions identified and only 2 (1.7%) patients required conversion to standard 4 port laparoscopic cholecystectomy. All patients were operated on in same day surgery with all except 2 (1.7%) being discharge home immediately following recovery from anesthesia. One admission was due to choledocholithiasis requiring further treatment, the other due to conversion to standard laparoscopic cholecystectomy secondary to local inflammation and adhesions. In addition, there were no SILS cholecystectomy mortalities and review of office follow up reveals no initial wound complications.
Conclusion
New innovative approaches to common surgical procedures must continue to demonstrate that they maintain sound surgical principles and safety in addition to equivalent to superior outcomes in comparison to the current standard of care. The results presented demonstrate that routine cholangiogram, an important tool in the general surgeon’s armamentarium for confirmation of biliary anatomy, is not sacrificed in any manner during SILS cholecystectomy. What’s more, it required little additional operative time to complete the procedure and had no associated complications.
Session Number: Poster – Poster Presentations
Program Number: P372
View Poster