Aayed R Alqahtani, FRCSC FACS, Mohamed Elahmedi, MD, Hussam Alamri, MD. King Saud University, College of Medicine, Department of Surgery
Introduction
Several studies questioned the long-term safety and efficacy of laparoscopic adjustable gastric banding (LAGB), primarily due to inadequate weight loss, weight regain, and band-related complications. The percentage of reoperations varies greatly, ranging from 2% to 80%. Although there is no consensus regarding which alternative surgical solution to perform, removal of the band, rebanding, conversion to gastric bypass, biliopancreatic diversion, and laparoscopic sleeve gastrectomy (LSG) have all been investigated as reoperative procedures, with varying degrees of success.
We conducted a retrospective review evaluating the feasibility of performing LSG at the time of band removal and assessing its safety and efficacy as a reoperative (Redo) solution.
Methods and Procedures
A retrospective review of patients who underwent LSG for poor outcome LAGB performed by a single surgeon between November 2007 and June 2011 was conducted. Data collection included patient demographics, weight and height at the time of banding and at 3, 6, 12, and 24 months post-gastric banding, complications, indication for revision, time interval between banding and Redo, weight and height at the day of reoperation, and at 3, 6, 12 and 24 months post-Redo. Hospital stay, operative time, and postoperative complications were also evaluated.
Results
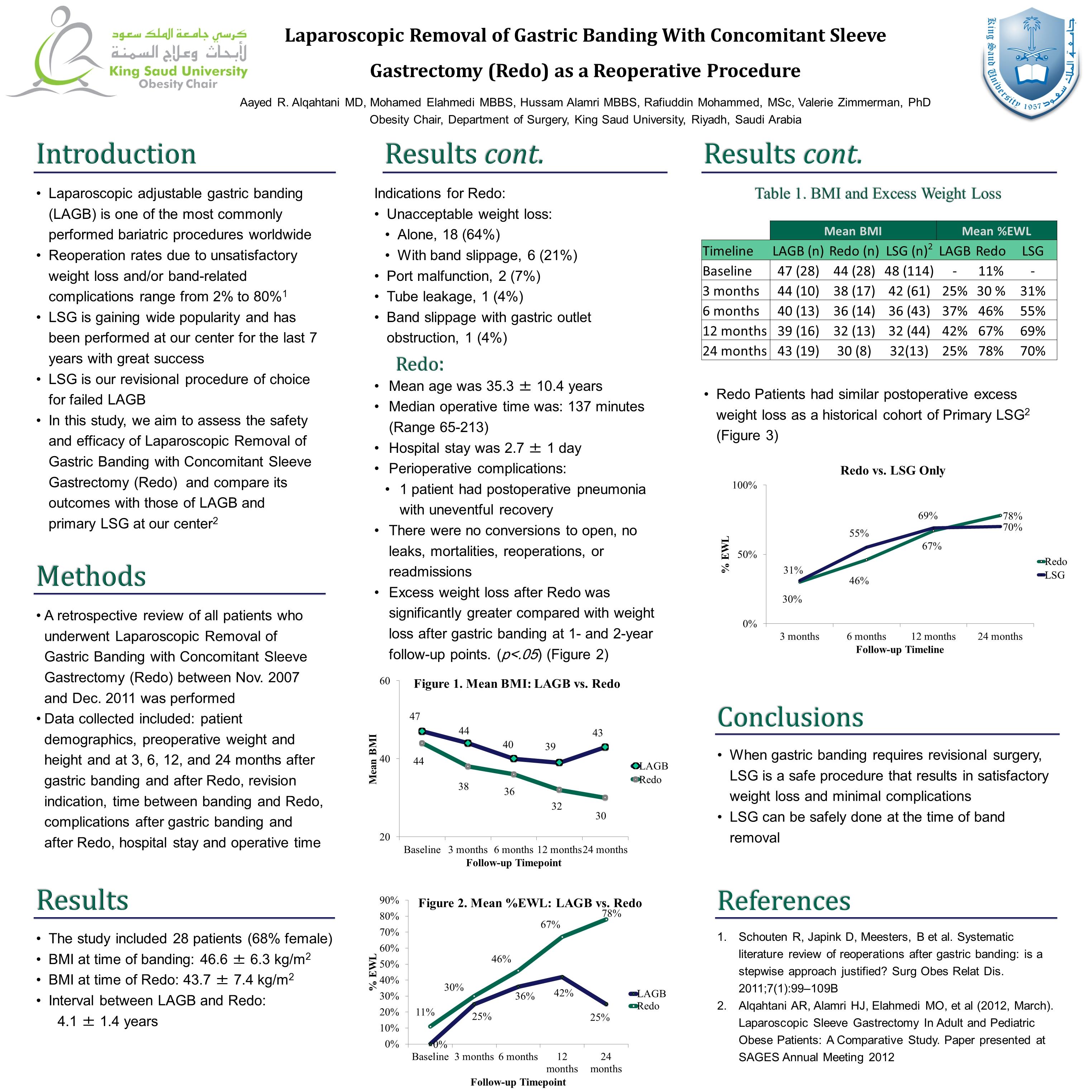
Twenty patients underwent LABG Redo during the study interval, of whom 13 were female (65%), with an average age of 28.3 ± 10.9 years . Median BMI was 49.6 kg/m2 (range 29.6-57.3) before band placement, and 41.6 kg/m2 (range 30.8-61.7) at the time of the revisional procedure, performed at an average of 3 years 5 months ± 1 year postoperative.
After gastric banding, 1 patient had gastric outlet obstruction secondary to band slippage, 4 had severe dysphagia, and 3 had intolerable reflux esophagitis. At 3, 6, 12, and 24 months post-gastric banding, patients had an excess BMI loss of 24.1%, 32.5%, 31.0%, and 22.7%, respectively. Nineteen patients (95%) had weight regain. After revisional surgery, excess BMI loss was 29.9%, 48.6%, 65.3%, and 69.2% at 3, 6, 12, and 24 months, respectively.
Mean operative time for the Redo surgery was 2 hours 25 minutes ± 36 minutes, and mean hospital stay was 2.6 ± 1.1 days. Following the Redo procedure, 1 patient had postoperative pneumonia with an uneventful recovery.
| Median BMI | Median Percentage Excess BMI Loss |
|
| Timeline | LAGB(n) Redo(n) | LAGB Redo |
| Baseline | 49.6 (20) 41.6 (20) | |
| 3 Months | 42.8 (10) 40.6 (13) | 24.1% 29.9% |
| 6 Months | 39.9 (13) 35.9 (14) | 32.5% 48.6% |
| 12 Months | 38.0 (15) 32.7 (10) | 31.0% 65.3% |
| 24 Months | 43.7 (11) 29.8 (6) | 22.7% 69.2% |
LAGB: Laparoscopic adjustable gastric banding
Redo: Laparoscopic removal of gastric banding with concomitant sleeve gastrectomy
Conclusion
Laparoscopic removal of gastric banding with concomitant sleeve gastrectomy is a safe and effective procedure, with higher excess BMI loss and fewer complications compared with LABG. LSG can be recommended as a revisional procedure for poor-outcome gastric banding.
Session Number: Poster – Poster Presentations
Program Number: P459
View Poster