Patrick R Reardon, MD, Brian J Dunkin, MD, Joanne M Chung, MD, Vadim Sherman, MD, Wega Koss, MD, Luis Benavente-Chenals, MD. The Methodist Hospital Department of Surgery Methodist Institute for Technology, Innovation, and Education Houston, Texas 77030
Background
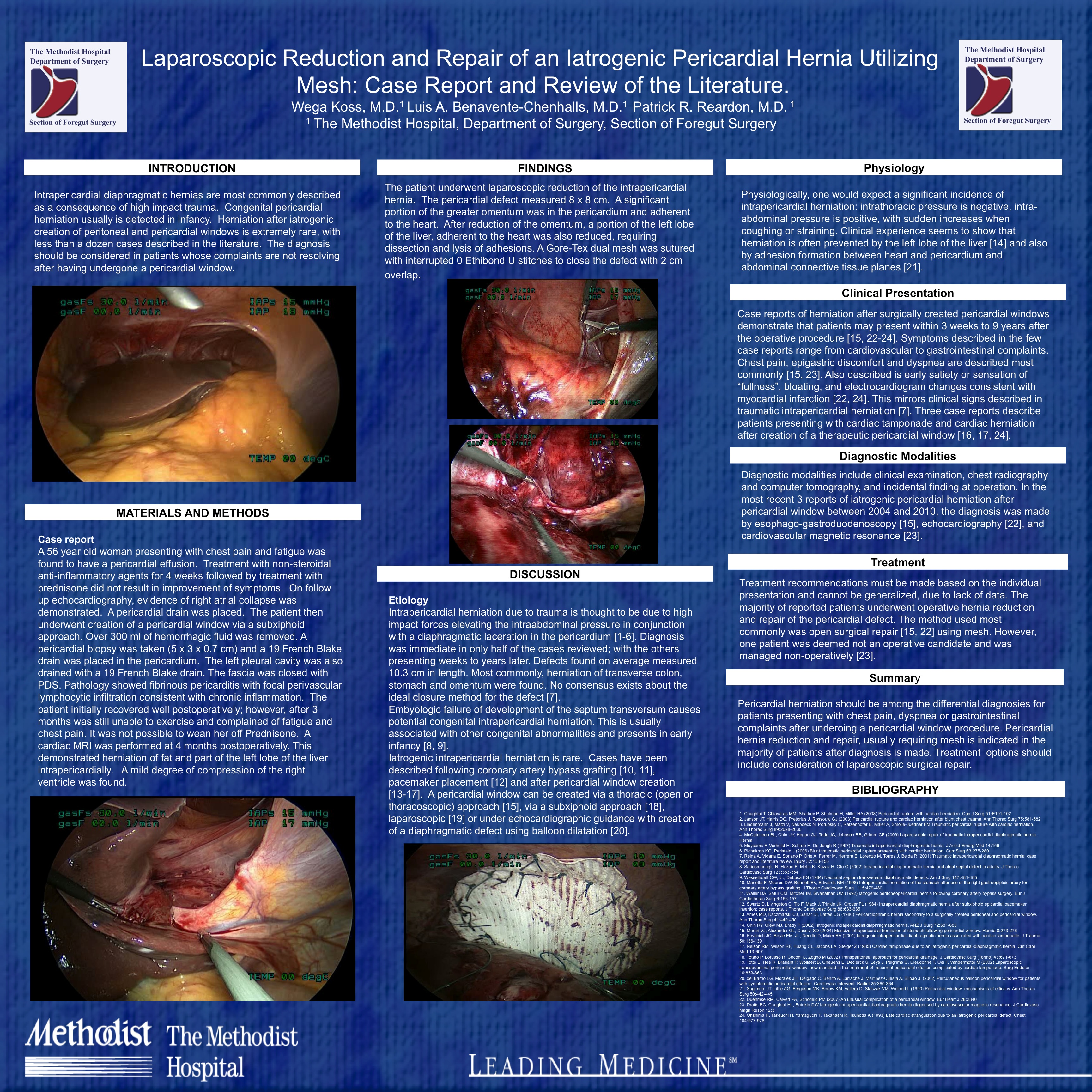
Intrapericardial diaphragmatic hernias are most commonly described as a consequence of high impact trauma. Congenital pericardial herniation usually is detected in infancy. Herniation after iatrogenic creation of peritoneal and pericardial windows is extremely rare, with less than a dozen cases described in the literature. The diagnosis should be considered in patients whose complaints are not resolving after having undergone a pericardial window procedure.
Methods
A 56 year old woman presenting with chest pain and fatigue was found to have a pericardial effusion. Treatment with non-steroidal anti-inflammatory agents for 4 weeks followed by treatment with prednisone did not result in improvement of symptoms. On follow up echocardiography, evidence of right atrial collapse was demonstrated. A pericardial drain was placed. The patient then underwent creation of a pericardial window via a subxiphoid approach. Over 300 ml of hemorrhagic fluid was removed. A pericardial biopsy was taken (5 x 3 x 0.7 cm) and a 19 French Blake drain was placed in the pericardium. The left pleural cavity was also drained with a 19 French Blake drain. The fascia was closed with PDS. Pathology showed fibrinous pericarditis with focal perivascular lymphocytic infiltration consistent with chronic inflammation. The patient initially recovered well postoperatively; however, after 3 months was still unable to exercise and complained of fatigue and chest pain. It was not possible to wean her off Prednisone. A cardiac MRI was performed at 4 months postoperatively. This demonstrated herniation of fat and part of the left lobe of the liver intrapericardially. A mild degree of compression of the right ventricle was found.
Results
The patient underwent laparoscopic reduction of the intrapericardial hernia. The pericardial defect measured 8 x 8 cm. A significant portion of the greater omentum was in the pericardium and adherent to the heart. After reduction of the omentum, a portion of the left lobe of the liver, adherent to the heart, was also reduced, requiring dissection and lysis of adhesions. The hernia defect was closed with interrupted U stitches of 0 braided polyester sutures affixing a polytetrafluoroethylene (Goretex) mesh to the diaphragmatic defect with at least 2 cm overlap in all directions. The postoperative course was uneventful.
Conclusions
Laparoscopic reduction and repair of an iatrogenic, incarcerated pericardial hernia utilizing mesh can safely and effectively be accomplished with excellent short-term outcomes.
Session: Poster
Program Number: P340
View Poster
{kind=link}