Joel F Bradley, MD, Kristopher B Williams, MD, Amanda L Walters, MS, B A Wormer, MD, K T Dacey, MHA, R F Sing, DO, K W Kercher, MD, B T Heniford, MD
Carolinas Medical Center
Introduction: The “July effect,” referring to worse patient outcomes at the start of the academic year, has been reported in medical literature and sensationalized by the media. The aim of this study was to analyze complex laparoscopic cases and assess whether such an effect exists in Minimally Invasive Surgery (MIS) fellowship training.
Methods: Data was analyzed for laparoscopic adrenalectomies, splenectomies and nephrectomies performed with MIS fellows at our institution from 2000-2011. Cases were designated as early (July-September) or late (March-May) for comparison. Patient demographics as well as outcome variables of operative time, complications, conversion to open, transfusion requirements and length of stay (LOS) were reviewed. Standard statistical analysis was performed.
Results: More than 500 cases were randomly sampled over the 11 years and reviewed; 197 solid organ resections met inclusion criteria. No differences were noted in age, gender, and BMI between early and late groups (p>0.05, Table 1). ASA scores (I, II, III, and IV) were evenly distributed between groups (p>0.05). When comparing operative outcomes between early and late cohorts, no differences were found in operative time, LOS, rate of blood or platelet transfusions required, and complications (Table 1), included pulmonary, infection, gastrointestinal, or cardiac problems. Major complications included cardiac dysrhythmias, pneumonia, readmission within 30 days, and septicemia. Conversion rates from laparoscopic to open were also similar (P>0.05, Table 1).
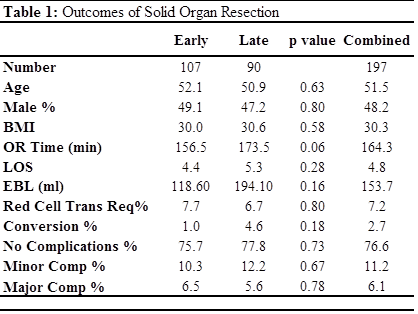
Conclusion: There is no difference in outcomes of advanced laparoscopic solid organ resection when performed in a fellowship program at the start or at the end of fellowship training. There is no July effect in surgical fellowships for solid organ surgery.
Session: Poster Presentation
Program Number: P596
